
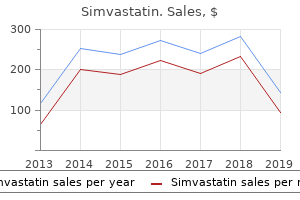
Simvastatin
"Buy simvastatin 10mg with mastercard, cholesterol test vancouver".
By: W. Luca, M.A., Ph.D.
Co-Director, George Washington University Medical School
It is always recommended to do an operative venogram to confirm that decompression operation has been successful cholesterol test where to go simvastatin 40mg free shipping. In extremely rare cases one may find webs at the junction of the subclavian vein and internal jugular vein cholesterol test how long for results buy cheap simvastatin 40 mg on line. This requires venotomy and excision of the web with subsequent closure of the venotomy of the subclavian vein lowering cholesterol foods eat purchase simvastatin 20mg online. Fibrinogen levels are often elevated in these patients and a hypercoagulable state has been postulated. The diseased artery is usually surrounded by a dense fibrotic reaction which incorporates the adjacent vein and less often the neighbouring nerve. Both upper and lower extremities are affected in contrast to arteriosclerosis which usually spares the upper extremities. In the lower extremities the disease generally occurs beyond the popliteal arteries, starting in tibial arteries extending to the vessels of the foot. In the upper extremities it is manifested by arterial involvement usually distal to the forearm in about 30% of patients. The acute lesion consists of acute arteritis and periarteritis, acute phlebitis and periphlebitis. In chronic lesion, the artery and the vein are bound together by fibrous adhesions. The internal and external elastic lamina of the artery are frequently much thickened. The typical patient is one who is a heavy smoker and had started smoking at an early age. In the upper extremity it is the vessels distal to the wrist that are involved so claudication is rare in upper extremity. Progression of ischaemia is similar to that in all chronic progressive arterial occlusions. Gradually postural colour changes appear, followed by trophic changes and eventually ulceration and gangrene of one or more digits and finally of the entire foot or hand requiring amputation. Some amelioration may be achieved by placing the affected limb in dependent position. One must remember of occasional involvement of the mesenteric or cerebrovascular circulation. The peculiar feature is that the ischaemic area is usually sharply demarkated with relatively good circulation in adjacent tissues. These include loss of hair from the digits, atrophy of the skin and brittle nails. Gradually there may be ulceration or gangrene of the toes commencing in the distal portion of the digit near the nail and gradually extend proximally to involve whole of the foot or hand. Absence of the posterior tibial pulse is highly suggestive of the diagnosis especially when bilateral. In the upper extremity the radial pulse may be absent and when bilateral it is also suggestive of this disease. So the characteristic arteriographic appearance of this disease is the smooth and normal appearance of larger arteries in combination with the extensive occlusion of the smaller arteries alongwith extensive collateral circulation. This included vasodilator drugs, anticoagulants, dextran, phenylbutazone and steroids. In these patients arterial reconstruction may be performed on the atherosclerotic proximal arteries, which in fact causes marked circulatory improvement. When gangrene is confined to a toe, amputation may be postponed, unless rest pain or infection is rather uncontrollable. When below-knee amputation can remove the gangrenous area, it will not be justified to go for above-knee amputation. In a few patients who stop smoking completely, progression of the disease is greatly restricted. Brachial plexus is formed by lower four cervical nerves (C5, 6, 7, 8) and the first thoracic nerve. When there is a very small contribution from the first thoracic nerve (Tl), this condition is known as prefixed brachial plexus. Sometimes the brachial plexus receives a big contribution from Tl and also a small part of T2. Such condition even with normal first thoracic rib, may cause symptoms similar to a cervical rib.
Close the anterior muscular layer with interrupted 4-0 atraumatic silk Lembert or Cushing sutures (Figs cholesterol kit walmart discount 40mg simvastatin free shipping. Insert this row of sutures about 6 mm away from the mucosal suture line to accomplish a certain amount of invag- ination of the rectum into the colon cholesterol test at home cvs buy simvastatin 20mg lowest price. Because the dimension of the side-to-end lumen is large cholesterol levels high risk buy simvastatin without prescription, narrowing does not result. After the anastomosis is completed, carefully inspect the posterior suture line for possible defects, which if present can be corrected by additional sutures. At this point cut the sutures and thoroughly irrigate the pelvis with a dilute solution of antibiotics. This omission has brought no noticeable ill effect, probably because the defect Fig. If there is, additional proximal colon Incise the previous scratch mark in the proximal colonic must be liberated. There must be sufficient slack that the segment with a scalpel and Metzenbaum scissors (Fig. If exposure is difficult, it is sometimes helpful to maintain Alternative to Colorectal Side-to-End gentle traction on the tails of the Cushing sutures to improve Anastomosis exposure while suturing the mucosa. Then cut the tails of the When the surgeon does not find it practicable to leave the Cushing sutures successively as the mucosal sutures are specimen attached to the rectal stump for purposes of traction inserted. Otherwise, cut all the Cushing sutures at one time, (the preferred technique described above), an alternative except for the two lateral guy sutures, which should be method may be used for the anastomosis. It is vitally important that the muscularis of the rec- der retractor deep to the prostate for exposure. Often the muscularis retracts Bring the previously prepared segment of descending 1 cm or more beyond the protruding rectal mucosa. The end of this seg- Bring the same needle back from inside out on the rectal ment of colon should have already been occluded by applica- stump and then from outside in on the proximal colon. When it is tied at antimesenteric border of the colon beginning 1 cm from the a later stage in the procedure, the knot lies on the mucosa of stapled end and continuing proximally for 4–5 cm, which is the colon. Place the second horizontal mattress suture halfway Insert a guy suture of atraumatic 4-0 silk from the left between the first suture and the left lateral guy suture by the lateral wall of the rectal stump to the termination of the inci- same technique. Grasp this suture in a hemostat without between the midpoint of the posterior layer and the right lat- tying it. Close the remainder of the posterior wall with interrupted The colon should slide down against the rectal stump horizontal mattress sutures of atraumatic 4-0 silk. Retaining the long tails of these stitches and apply- ing mild upward traction improve the exposure for insertion Fig. The remainder of the anastomosis is similar to that described above for the Baker technique. For tumors situated 6–9 cm above the anal rectum about 1 cm beyond the lower edge of the tumor. Then verge, it is necessary to dissect the rectum down to the leva- divide the upper colon between Allen clamps at the site pre- tor diaphragm, which requires complete division of viously selected for this purpose. Ligate the cut distal end of Waldeyer’s fascia posteriorly, dissection of the anterior rec- the descending colon with umbilical tape, and cover it with a tum away from the prostate to the level of the urethra, and sterile rubber glove (Fig. There should be sufficient slack Unless the patient has a narrow pelvis, the entire leva- in the colon to fill the hollow of the sacrum on its way to the tor diaphragm then comes into view (Fig. If not, liberate the transverse colon to the perirectal lymphatics readily peel off the levator mus- achieve sufficient slack. Then follow the posterior wall of the rectum Next, remove the Allen clamp and gently dilate the colon down to the puborectalis muscle, which marks the cepha- with appropriate sizers or a Foley catheter balloon. Take care not to continue dis- the colon may prove the most frustrating step of the entire secting beyond the puborectalis, as it is easy to enter the operation. Be careful not to produce any serosal tears during intersphincteric plane and liberate the rectum down to the this maneuver. Ascertain that all fat and mesen- whipstitch after the specimen has been detached because the tery have been dissected off the distal 1. Each bite should in the staple line, firing the stapler may produce significant contain 4 mm of full-thickness rectal wall, and the stitches bleeding in the rectal lumen, which is difficult to control.
Unlike other pathogens afecting cystic fbrosis site and the vessels causing hemoptysis cholesterol levels vegetarian diet purchase simvastatin online from canada. Anomalous systemic arterial supply to the basal tent patients xanthelasma/ cholesterol eyelid deposits simvastatin 20 mg low price, causing chronic suppurative otitis media com- segments of the right lower lobe in neonate cholesterol test how accurate generic simvastatin 10mg. Pulmonary lobar atelectasis with high-density glands due to defect in the permeability of epithelium to materials seen within the bronchi can be due to chloride ions. Median survival age is attenuation is due to calcium oxalate crystal 29 years, and up to 95 % of deaths are due to progressive pul- deposition within the plugs for unknown reason. Te defec- tive ciliary mechanism within the bronchial tree causes the pulmonary secretions to accumulate within the terminal bronchioles (mucus plugs). Retention cysts in contrast are due to blockage of a mucous gland duct, not the sinus itself. Up to 70 % of mucoceles are located in the frontal and the ethmoid sinuses (maxillary mucocele is rare). Patients with mucocele can present with proptosis and unilateral visual disturbance if the mucocele presses over the globe and the optic pathways. When the mucocele is infected, it is called pyocele and pres- ents clinically with fever and pain. Mucoceles are detected as complete sinus opacification with expansion of the affected sinus. Most complaints are due to unilateral or bilateral nasal destruction of the fine air cell bony septations blockage (81%), rhinorrhea (50%), daily headache (51%), (differentiate it from mucocele). Tey commonly arise secondary to chronic with thinning and expansion of the sinus walls. Pyocele can cele is a slow-growing, expansile, cyst-like mass within the show hyperdense mass with air inclusions. Abdominal punctuated or plaque-like calcifications center will not enhance as high as the normal mucosa. If the mucocele contains hemorrhage, then it will show high signal intensity in all pulses. Intussusception is seen as a “donut appearance” mass with hypoechoic rim and echogenic center. Pancreatic insufciency is common due to the inherent ducts with ductal proliferation and hyperplasia. Multiple scattered areas of fatty infiltration can be to bicarbonate and water secretion. Pancreatic insufciency arises due to pan- hyperechoic fatty masses with hypoechoic rim and creatic fatty replacement, cystic changes, and pancreatic can be easily mistaken for abnormal liver masses. Colonic wall redundancy is detected as hypertrophic sis, biliary cirrhosis (30 %), portal hypertension, and spleno- colonic wall folds (>4 mm) with overlapping. In older children, intestinal obstruction can occur due complete replacement of the pancreas with fat with to fecal and colonic fecal impaction (distal intestinal obstruc- high-attenuation pancreatic duct within it can be tion syndrome ). Te colon shows marked strictures, within the pancreas due to inspissation of proteins in longitudinal shortening, and loss of the haustra due to muco- the acini and ductules, causing their dilatation and sal fbrosis and thickening of the muscularis mucosa. Pseudomasses are seen as multiple 318 Chapter 7 · Pulmonology hypodense masses with fat attenuation surrounded by normal liver parenchyma. On axial view, intussusception shows “target sign” with crescent hypodense area inside it representing the mesentery. Enhancing mesenteric vessels within the mass is frequently seen (very characteristic;. On longitudinal axis, the intussusception is seen as an area of “sausage-shaped” mass. The contrast makes a rim around the area of the intussusception due to bowel invagination. Colonic wall redundancy shows overlapping colonic folds, producing a double or triple appearance of the wall mimicking wrinkles (. Hyperdensity areas within the wall before contrast injection may be 7 seen due to inspissated mucofeculent material. After contrast injection, the inner wall shows marked enhancement due to hypervascularity. Testicular microlithiasis is a condition characterized by the presence of multiple punctuated 1–3 mm calcifcations within the testicular parenchyma.
One layer of interrupted • Findings 4-0 Vicryl sutures is used for this anastomosis cholesterol definition in hindi discount 20mg simvastatin fast delivery. Insert the • End-to-side versus side-to-side anastomosis first stitch of the posterior layer approximating the mid- point of the duodenal incision to the distal margin of the choledochotomy cholesterol levels eating before test purchase 20mg simvastatin with visa. A right subcostal or a midline incision from the xiphoid Approximate the proximal margin of the choledochotomy to a point 5 cm below the umbilicus is suitable for with the same suture material to the midpoint of the ante- this operation kresser cholesterol ratio purchase simvastatin from india. Divide any adhesions and explore the rior layer of the duodenum and tie this stitch so it inverts 83 Choledochoduodenostomy: Surgical Legacy Technique 751 Fig. In this case, enlarge the choledochotomy so it measures at least the mucosa of the duodenum (Fig. Make an incision in the duodenum parallel to the choledochotomy and approximately equal in length (Fig. Leave the tails of the most cephalad and most distal sutures long, but cut all other sutures. The knots are on the outside surface of the anastomosis for Postoperative Care the anterior layer. Drainage and Closure Complications As bile has an extremely low surface tension, there is a Duodenal fistula (see Chap. Choledochoduodenostomy: importance of common duct size and occurrence of cholangitis. Choledochoduodenostomy: an 18 year study of 175 Qadan M, Clarke S, Morrow E, Triadafilopoulos G, Visser B. Either the end of the Roux limb (please see section below on Side-to-end Biliary reconstruction after major ductal injury Choledochojejunostomy or Hepaticojejunostomy) or the side Common bile duct obstruction due to nonresectable tumor, may be used. This type of anastomosis is commonly performed Preoperative Preparation for palliation of carcinoma of the pancreas, when endoscopic stenting fails or is not technically feasible. The anastomosis is commonly performed for operative stric- Devascularizing the jejunal segment by inaccurate division tures or injuries. In most cases, the marginal artery of the jejunum is divided immediately distal to the artery supplying An isoperistaltic Roux-en-Y segment of jejunum provides a the second arcade. By dividing only one or two additional safe way to drain the extrahepatic biliary tract. There are sev- arcade vessels, sufficient jejunum can be mobilized to reach eral ways to construct the anastomosis to the bile duct. The jejunum is passed to-end or side-to-side choledochojejunostomy are equivalent through an incision in the avascular portion of the transverse and has the advantage of simplicity. Circumferential dis- mesocolon, generally to the right of the middle colic artery. Chassin When a Roux-en-Y biliary-intestinal bypass is performed Which Type of Bypass? Some pancre- For carcinoma of the pancreas, evaluate the local extent of atic tumors extend deeply into this mesentery, making it disease and its probable future encroachment on the common impossible to separate the jejunal blood supply for the Roux- duct, cystic duct, and root of the jejunal mesentery. This operation is contraindicated in these few sive disease limits access to the common duct or involves the cases, and some other type of bypass must be considered. A cholangiogram, obtained through the cys- • Findings tic duct, may help operative planning and is easy to obtain. Operative Technique Creating the Roux-en-Y Jejunal Limb Incision and Biopsy Once it is decided to proceed with a Roux-en-Y bypass, divide the jejunum and its mesentery. Inspect the proximal If there has been a previous operation on the biliary tract that jejunal mesentery and look for the first two branches from utilized a subcostal incision, make a long midline incision. If the superior mesenteric artery to the jejunum just beyond the the previous incision was vertical, make a long subcostal ligament of Treitz. In secondary cases, the first 2 cm beyond its junction with the second jejunal branch, effort is to free the peritoneum of the anterior abdominal wall which is generally about 15 cm from the ligament of Treitz. Then continue to free the structures as described in the jejunum across the marginal artery and into the avascular Chap. Divide the mesentery in a distal direc- With primary operations for carcinoma of the pancreas, tion until the third vessel is encountered. Divide and ligate make a long midline incision from the xiphoid to a point this vessel and continue the incision in the mesentery down 6–7 cm below the umbilicus. This most often does not require division bypass or for partial or total pancreatectomy. In Clean the mesenteric margin of the jejunum and divide patients with inoperable pancreatic carcinoma, take biopsy between Allen clamps or with a cutting linear gastrointesti- specimens from areas of obvious carcinoma with a scalpel nal stapler.
Generic 20mg simvastatin with amex. Sanjeevani || ASHTHMA HIGH BP Heart Disease Cholesterol .