
Nootropil
"Purchase nootropil 800 mg on-line, medicine cabinet".
By: O. Khabir, M.A.S., M.D.
Co-Director, Dell Medical School at The University of Texas at Austin
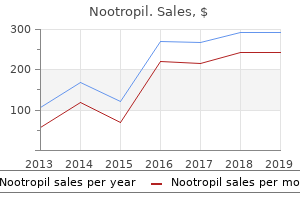
Sucrase converts the disaccharide sucrose (table sugar) to glucose and Enzymes are proteins that catalyze fructose treatment interventions cheapest nootropil, and lactase converts the disaccharide lactose (milk sugar) to glucose biochemical reactions symptoms torn rotator cuff cheap nootropil 800mg overnight delivery; in other and galactose medicinenetcom symptoms nootropil 800mg low cost. Monosaccharides produced by digestion and dietary monosaccha- words, they increase the speed at rides are absorbed by the intestinal epithelial cells and released into the hepatic which reactions occur. Their names usually portal vein, which carries them to the liver. Proteins Proteins are amino acids linked Dietary proteins are cleaved to amino acids by proteases (see Fig. Dipeptides Pepsin acts in the stomach, and the proteolytic enzymes produced by the pancreas have two amino acids, tripeptides (trypsin, chymotrypsin, elastase, and the carboxypeptidases) act in the lumen of the have three amino acids, and so on. Aminopeptidases and di- and tripeptidases associated with the intes- proteases are enzymes that cleave the pep- tinal epithelial cells complete the conversion of dietary proteins to amino acids, tide bonds between the amino acids (see which are absorbed into the intestinal epithelial cells and released into the hepatic Chap. Fats Fats must be transported in the The digestion of fats is more complex than that of carbohydrates or proteins blood bound to protein or in because they are not very soluble in water. The triacylglycerols of the diet are lipoprotein complexes because emulsified in the intestine by bile salts, which are synthesized in the liver and they are insoluble in water. Pancreatic lipase converts the triacylglycerols in the cylglycerols and cholesterol are found in lumen of the intestine to fatty acids and 2-monoacylglycerols (glycerol with a lipoprotein complexes. The fatty acids and 2-monoacylglycerols are absorbed from these micelles into the intestinal epithelial cells, where they are The laboratory studies ordered at resynthesized into triacylglycerols. The triacylglycerols are packaged with pro- the time of his second office visit show that Ivan Applebod has teins, phospholipids, cholesterol, and other compounds into the lipoprotein com- hyperglycemia, an elevation of blood glu- plexes known as chylomicrons, which are secreted into the lymph and ultimately cose above normal values. CHANGES IN HORMONE LEVELS AFTER A MEAL hours after a meal, when glucose should have been taken up by tissues and blood After a typical high carbohydrate meal, the pancreas is stimulated to release the glucose returned to the fasting level, approx- hormone insulin, and release of the hormone glucagon is inhibited (see Fig. Endocrine hormones are released from endocrine glands, such as the determined after an overnight fast was 162 pancreas, in response to a specific stimulus. Because both of these blood glucose messages between tissues concerning the overall physiologic state of the body. The endocrine hormone insulin, which is formerly known as non–insulin-dependent secreted from the pancreas in response to a high-carbohydrate meal, carries the diabetes mellitus (NIDDM), was made. In message that dietary glucose is available and can be used and stored. The this disease, liver, muscle, and adipose tis- sue are relatively resistant to the action of release of another hormone, glucagon, is suppressed by glucose and insulin. The subsequent changes in circulating hormone levels cause glycerols. Therefore, more glucose remains changes in the body’s metabolic patterns, involving a number of different tis- in his blood. Conversion to Glycogen, Triacylglycerols, and CO2 in the Liver Because glucose leaves the intestine via the hepatic portal vein, the liver is the first tissue it passes through. The liver extracts a portion of this glucose from the blood. Some of the glucose that enters hepatocytes (liver cells) is oxidized in adenosine triphosphate (ATP)-generating pathways to meet the immediate energy needs of these cells and the remainder is converted to glycogen and triacylglycerols or used for biosynthetic reactions. In the liver, insulin promotes the uptake of glucose by increasing its use as a fuel and its storage as glycogen and triacylglycerols (see Fig. As glucose is being oxidized to CO , it is first oxidized to pyruvate in the path- In the liver and most other tissues, 2 glucose, fats, and other fuels are oxi- way of glycolysis. The acetyl group enters dized to the 2-carbon acetyl group the tricarboxylic acid (TCA) cycle, where it is completely oxidized to CO2. Energy O from the oxidative reactions is used to generate ATP. Liver glycogen stores reach a maximum of approximately 200 to 300 g after a CH3 C of acetyl CoA. CoA, which makes the acetyl group high-carbohydrate meal, whereas the body’s fat stores are relatively limitless. As the more reactive, is a cofactor (coenzyme A) glycogen stores begin to fill, the liver also begins converting some of the excess glu- derived from the vitamin pantothenate.
The child was placed back on the operating table and a short 30-minute procedure was per- formed to revise the rod symptoms 2016 flu order 800mg nootropil with visa. At the end of this short revision treatment 4 hiv discount nootropil 800mg otc, the patient had a sudden drop of blood pressure and there was also extensive bleeding from the surgical site symptoms 2 months pregnant best order nootropil. It was concluded at this time that the child was in a coagu- lopathy, and aggressive resuscitation with blood products was begun. Dur- ing the time, the child was moved back over to the hospital bed, the arterial line became dislodged, and it was some time before it was possible to get fur- ther blood pressure readings. During this time the child had a severe hypo- tensive event and continued with bleeding. The child was resuscitated and taken to the intensive care unit but continued to bleed into the chest; how- ever, the mother requested that no further resuscitation be performed. In an- other case, the child had a very uneventful anterior and posterior procedure with exceptionally low blood loss. Again, the child was transferred to the hospital bed. Some time was consumed in obtaining appropriate radio- graphs, and over a 30- to 45-minute period, the child was transferred to the intensive care unit. As the child was being moved into the intensive care unit, the portable monitor showed that the blood pressure had dropped and there was a concern that there might have been a monitor malfunction; however, 9. Spine 467 with a short review, it was determined that the child had a cardiac arrest. The child was then returned to the operating room, aggressively resuscitated, and returned to the intensive care unit. No source of bleeding was found and the cardiac arrest was due to a combination of hypovolemia and anemia. Again, the mother requested that no further resuscitation efforts be made, and 8 hours later, the child had another drop in blood pressure and a car- diac arrest and no resuscitation was performed. These two cases demonstrate the extreme importance of maintaining a high state of vigilance in this pe- riod from the end of the operative procedure until children are safely in the intensive care unit with full monitoring. Immediate Postoperative Period Immediate postoperative deaths may occur if there is not an aggressive in- tensive care unit management of electrolyte balance, coagulopathy, hypov- olemia, and respiratory support. We had one death in the first 24 hours after surgery in which the girl developed a rapid coagulopathy followed by a car- diac arrest from which she could not be resuscitated. The postmortem examination showed severe hemorrhagic pancreatitis for which there was no explanation for the cause. Risks of death after the acute postoperative period are mainly due to respiratory compromise. After discharge from the hospital, the risk may be higher in the first 6 months, but not substantially. Again, this risk involves those children with the most severe neurologic dis- ability. We also had three deaths of children who were scheduled for surgery but died before the spine surgery could be performed. All of these were se- verely involved children in whom the caretakers noted increasing problems from the scoliosis and desired aggressive comfort management. The treating physician did not perceive that these children were having any more medical problems than many similar children who do well and make significant improvements following surgery. We also had three children die in the first 3 months after surgery after discharge from the hospital. One of these chil- dren was admitted to the hospital with what was initially thought to be se- vere constipation; however, she quickly became septic and was believed to have an acute surgical abdomen. The family refused surgical treatment of the acute abdomen because the spinal fusion had been performed under a no re- suscitation order. When the child died, the postmortem examination showed a ruptured Meckel’s diverticulum that was completely unrelated to the spinal fusion. Another child developed pneumonia 6 weeks after discharge and was admitted to another hospital, where again the family refused to have the child intubated, and she died. The spinal fusion may have been related in the development of her pneumonia; however, one of the goals of the spine surgery was to try to improve her res- piratory function, which had been getting progressively worse. A third child was found dead in bed in the morning by the caretaker 4 weeks after dis- charge.
Buy generic nootropil on line. Withdrawing from herion. Day 1.
This cycle cannot be converted to glucose as enzyme treatment knee pain proven 800mg nootropil, which requires biotin medicine bottle buy nootropil us, is the catalyst of an anaplerotic (refilling) reaction readily medications used to treat bipolar disorder 800mg nootropil. In gluconeogenesis, this reaction replenishes the oxaloacetate that is used for the synthesis of glucose (Fig. The CO2 that was added to pyruvate to form oxaloacetate is released in the reac- tion catalyzed by phosphoenolpyruvate carboxykinase (PEPCK), which generates PEP (Fig. For this reaction, GTP provides a source of energy as well as the phosphate group of PEP. In various species, PEPCK is located either in the cytosol or in mitochondria, or it is distrib- uted between these two compartments. In humans, the enzyme is distributed about equally in each compartment. Oxaloacetate, generated from pyruvate by pyruvate carboxylase or from amino acids that form intermediates of the TCA cycle, does not readily cross the mito- chondrial membrane. It is either decarboxylated to form PEP by the mitochondrial PEPCK or it is converted to malate or aspartate (see Figs. The Only the three carbons at the - conversion of oxaloacetate to malate requires NADH. PEP, malate, and aspartate end of an odd chain fatty acid that can be transported into the cytosol. The remaining 16 carbons of a ers of oxaloacetate) and enter the cytosol, they are reconverted to oxaloacetate by fatty acid with 19 carbons form acetyl CoA, reversal of the reactions given above (see Figs. The conversion of which does not form any net glucose. Whether oxaloacetate is transported CHAPTER 31 / GLUCONEOGENESIS AND MAINTENANCE OF BLOOD GLUCOSE LEVELS 563 Glucose PEP Cytosol 4 CO2 + Glucagon via cAMP phosphoenol– pyruvate carboxykinase GDP ADP pyruvate inactive kinase (PK) PK– P GTP ATP Alanine OAA Pyruvate 1 NADH Lactate + NADH + NAD NAD Asp Malate Adipose 3 Pyruvate TG 2 CO2 + Glucagon via cAMP pyruvate carboxylase Biotin ATP FA – ADP Asp OAA Pi NADH 1 NADH pyruvate FA 2 dehydrogenase + NAD + Activated by – Inhibited by Malate Acetyl CoA Mitochondrion Inducible enzyme Inactive enzyme Ketone bodies OAA exits from the mitochondrion either as aspartate or malate1 2 Fig. Conversion of pyruvate to phosphoenolpyruvate (PEP). Follow the shaded circled numbers on the diagram, starting with the precursors alanine and lactate. The first step is the conversion of alanine and lactate to pyruvate. Pyruvate then enters the mitochondria and is converted to OAA (circle 2) by pyruvate carboxylase. Pyruvate dehydrogenase has been inactivated by both the NADH and acetyl-CoA generated from fatty acid oxidation, which allows oxaloacetate production for gluconeogenesis. The oxaloacetate formed in the mitochondria is converted to either malate or aspartate to enter the cytoplasm via the malate/aspartate shuttle. Once in the cytoplasm the malate or aspartate is converted back into oxaloacetate (circle 3), and phosphoenolpyruvate carboxykinase will convert it to PEP (circle 4). The white circled numbers are alternate routes for exit of carbon from the mitochondrion using the malate/aspartate shuttle. OAA oxaloacetate; FA fatty acid; TG triacylglycerol. NADH is required to reduce 1,3-bisphospho- glycerate to glyceraldehyde 3-phosphate during gluconeogenesis. Oxaloacetate, produced from malate or aspartate in the cytosol, is converted to PEP by the cytosolic PEPCK (see Fig. CONVERSION OF PHOSPHOENOLPYRUVATE TO FRUCTOSE C 1,6-BISPHOSPHATE Biotin COO– pyruvate carboxylase COO– The remaining steps of gluconeogenesis occur in the cytosol (Fig. Starting Pyruvate Oxaloacetate with PEP as a substrate, the steps of glycolysis are reversed to form glyceraldehyde 3-phosphate. For every two molecules of glyceraldehyde 3-phosphate that are Fig. Conversion of pyruvate to oxaloac- formed, one is converted to dihydroxyacetone phosphate (DHAP). The generation of PEP from gluconeogenic precursors.
Of the wide variety of enzymes that are involved in xenobiotic metab- olism medicine website discount 800 mg nootropil free shipping, only the cytochrome P450–dependent monooxygenase system is discussed Table 46 treatment gout buy nootropil paypal. The cytochrome P450–dependent monooxygenase enzymes are determi- Used in Biotransformation of Xenobiotic Compounds nants in oxidative medications medicare covers buy generic nootropil canada, peroxidative, and reductive degradation of exogenous (chemi- Acetyltransferase cals, carcinogens, and pollutants, etc. The key enzymatic constituents of this system are the flavo NADPH NADP+, H+ protein NADPH-cytochrome P450 oxidoreductase and cytochrome P450 (Fig. The latter is the terminal electron acceptor and substrate-binding site of the microso- FAD mal mixed-function oxidase complex, a very versatile catalytic system. The system – – RH O2 ROH, H2O got its name in 1962, when Omura and Sato found a pigment with unique spectral e e characteristics derived from liver microsome of rabbits. When reduced and complexed FMN with carbon monoxide, it exhibited a spectral absorbance maximum at 450 nm. The major role of the cytochrome P450 enzymes (see Chapter 25) is to oxidize Fe–heme substrates and introduce oxygen to the structure. Similar reactions can be carried out by other flavin monoxygenases that do not contain cytochrome P450. The cytochrome P450 enzyme family contains at least 100 to 150 different isozymes with at least 40% sequence homology. These isozymes have different but Cytochrome Cytochrome overlapping specificities. The human enzymes are generally divided into six major P450 reductase P450 subfamilies, and each of these is further subdivided. General structure of the P450 the principal enzyme involved in the oxidation of ethanol to acetaldehyde, CYP2E1, enzymes. O binds to the P450 Fe-heme in the 2 the CYP denotes the cytochrome P450 family, the 2 denotes the subfamily, the E active site and is activated to a reactive form by denotes ethanol, and the 1 denotes the specific isozyme. The electrons are donated The CYP3A4 isoform accounts for 60% of CYP450 enzymes in the liver and by the cytochrome P450 reductase, which con- 70% of cytochrome enzymes in gut wall enterocytes. It metabolizes the greatest tains an FAD plus an FMN or Fe-S center to number of drugs in humans. The con- facilitate the transfer of single electrons from comitant ingestion of two CYP3A4 substrates could potentially induce competition NADPH to O2. The P450 enzymes involved in for the binding site, which, in turn, could alter the blood levels of these two agents. For CYP2E1, RH is ethanol The drug with the highest affinity for the enzyme would be preferentially metabo- (CH3CH2OH), and ROH is acetaldehyde lized, whereas the metabolism (and degradation) of the other drug would be (CH3COH). The latter drug’s concentration in the blood would then rise. Moreover, many substances or drugs impair or inhibit the activity of the CYP3A4 enzyme, thereby impairing the body’s ability to metabolize a drug. The lipid-lowering agents known as the statins (HMGCoA reductase inhibitors) require CYP3A4 for degradation. Appropriate drug treatment and dosing takes into account the normal degradative pathway of the drug. However, grapefruit juice is a potent inhibitor of CYP3A4-mediated drug metabolism. Evidence suggests that if a statin is regularly taken with grapefruit juice, its level in the blood may increase as much as 15-fold. This marked increase in plasma concentration could increase the muscle and liver toxicity of the statin in question. The cytochrome P450 isozymes all have certain features in common: 1. They all contain cytochrome P450, oxidize the substrate, and reduce oxygen. They all have a flavin-containing reductase subunit that uses NADPH, and not NADH, as a substrate.