
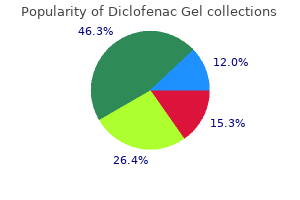
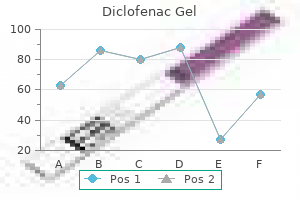
Diclofenac Gel
"Order diclofenac gel online from canada, arthritis diet and activity promotion trial".
By: W. Saturas, M.A., M.D., Ph.D.
Deputy Director, Marian University College of Osteopathic Medicine
Sulindac is one exception in that its sulfide metabolite is the active form of the drug and has a half-life of 16 hours [35] painkillers for arthritis in the knee proven 20 gm diclofenac gel. Nabumetone is also a prodrug arthritis in back of head discount diclofenac gel online american express, and its active metabolite arthritis knee treatment ice cheap 20 gm diclofenac gel visa, 6-methoxy-2-naphthylacetic acid, has a half-life of more than 20 hours (and even longer in the elderly) [36]. Indomethacin, sulindac, etodolac, piroxicam, carprofen, and meloxicam undergo enterohepatic recirculation [35,37,38]. In contrast to salicylate poisoning, the acidosis that sometimes occurs with large overdoses of these agents appears to be due to high levels of parent drug and metabolites rather than to disruption of metabolism [39]. It most commonly results from ingestion, but poisoning due to topical use [47] and rectal self-administration [48] has been reported. The ingestion of topical preparations of methyl salicylate (oil of wintergreen, also present in Chinese propriety medicines) can result in rapid-onset poisoning, due to its concentration, rapid absorption kinetics, and higher lipid solubility. Infants may become poisoned by ingesting the breast milk of women chronically taking therapeutic doses of salicylate [49]. Intrauterine fetal demise resulting from poisoning during pregnancy [50] and neonatal poisoning resulting from the transplacental diffusion of therapeutic doses of salicylate taken before delivery [51] have also been described. Regardless of whether poisoning is acute or chronic, it can be characterized as mild, moderate, or severe on the basis of the serum pH and underlying acid–base disturbance (Table 122. This approach was first described in the classic papers by Done [40,54], who also developed a nomogram that attempted to correlate the severity of poisoning with a timed salicylate level after acute ingestion. Although Done’s nomogram has subsequently been shown to have poor predictive value [41,52], his observation that the clinical severity of poisoning correlates with acid– base status remains undisputed. It may develop 2 to 8 hours after acute ingestion of 150 to 300 mg per kg of aspirin [40,54] or any time during chronic therapy. Associated signs and symptoms include nausea, vomiting, abdominal pain, headache, tinnitus, tachypnea (or subtle hyperpnea), ataxia, dizziness, agitation, and lethargy. The anion gap (see Chapter 198) is normal until late in this stage, when compensatory renal bicarbonate excretion eventually lowers the serum bicarbonate level. Despite total body fluid and electrolyte depletion and clinical dehydration, laboratory evidence of dehydration (e. It may also occur in patients with chronic ingestion who delay seeking medical care for symptoms of mild poisoning and continue to take salicylate. There may be agitation, asterixis, diaphoresis, deafness, pallor, confusion, slurred speech, disorientation, hallucinations, tachycardia, tachypnea, and orthostatic hypotension. It can occur 6 to 24 hours or more after the acute ingestion of more than 500 mg per kg of aspirin [40,54] or in unrecognized or untreated chronic poisoning. Other findings may include coma, seizures, papilledema, hypotension, dysrhythmias, congestive heart failure, oliguria, hypothermia or hyperthermia, rhabdomyolysis, and multiple organ failure [46,53,55]. Asystole is the most common terminal dysrhythmia, but ventricular tachycardia and ventricular fibrillation can also occur [45,46,56,57]. Although an increased anion-gap metabolic acidosis is often said to be a hallmark of salicylate poisoning, in reality a variety of acid–base disturbances may be seen depending on the delay to presentation and severity of poisoning. In adults, combined respiratory alkalosis and metabolic acidosis is the most common finding (50% to 61%), followed by pure respiratory alkalosis (20% to 25%), pure metabolic acidosis (15% to 20%), and a combined respiratory and metabolic acidosis (5%) [28,46]. Metabolic acidosis is more common and respiratory alkalosis more often absent in children than in adults [42,46] suggesting that children progress more rapidly from mild to severe poisoning, perhaps because of more rapid and extensive tissue distribution of drug [58]. Metabolic acidosis is also more common in patients with large acute ingestions, chronic intoxication, and delayed presentation or treatment [28,42,43,46,59]. The onset and progression of toxicity may be delayed after overdose with enteric-coated or sustained-release formulations [17]. Potential complications of both therapeutic and toxic doses of salicylate include gastrointestinal tract bleeding, increased prothrombin time, hepatic toxicity, pancreatitis, proteinuria, and abnormal urinary sediment. Significant bleeding, gastrointestinal tract perforation, blindness, and inappropriate secretion of antidiuretic hormone are rare complications of acute poisoning. Other Nonsteroidal Anti-Inflammatory Drugs With the exception of mefenamic acid and phenylbutazone, significant toxicity from acute overdose is unusual and occurs following massive ingestion. Manifestations typically include nausea, vomiting, abdominal pain, headache, confusion, tinnitus, drowsiness, and hyperventilation [5,60,61]. Symptoms rarely last more than several hours, and acute renal toxicity is almost always reversible over a period of a few days to weeks. Metabolic acidosis, coma, seizures, hepatic dysfunction, hypotension, and cardiovascular collapse are relatively frequent after phenylbutazone overdose [60,61,64–66]. Uncommonly, coma, hyperactivity, hypothermia, seizures, metabolic acidosis, acute renal insufficiency, thrombocytopenia, acute respiratory distress syndrome, upper gastrointestinal tract bleeding, and respiratory depression are seen in ibuprofen poisoning [39,66–69].
Additional information:
However rheumatoid arthritis knee icd 9 buy genuine diclofenac gel online, inhaled ipratropium bromide currently is not recommended for routine use once a patient is hospitalized with a severe exacerbation of asthma [1 arthritis in the knee running purchase generic diclofenac gel online,2] arthritis in back and neck symptoms order diclofenac gel once a day. The long-acting anticholinergic, tiotropium, has a role in treating outpatients with difficult to control asthma, but it does not have any established role for treating hospitalized patients with acute exacerbations of asthma [1,2,67]. Methylxanthines Because the literature does not demonstrate a benefit to adding methylxanthines to β2-adrenergic agonists in the acute setting and because they increase toxicity, methylxanthines are no longer recommended for the treatment of asthma exacerbations [1,2,68–70]. For the rare, critically ill patient whose condition is acutely deteriorating despite maximal recommended therapy with bronchodilators, corticosteroids, and other adjuncts [1,2], the use of methylxanthines might be considered by some physicians, although data are not supportive [71]. For patients not already taking methylxanthines, a loading dose of aminophylline (6 mg/kg lean body weight) can be administered over 20 to 30 minutes, followed by an intravenous infusion at the rate of 0. This infusion rate should be decreased when conditions are present that decrease methylxanthine clearance, especially congestive heart failure, cirrhosis, and the use of drugs such as cimetidine, ranitidine, allopurinol, oral contraceptives, erythromycin, ciprofloxacin, or norfloxacin. Six hours after initiation of the infusion, the serum theophylline level should be checked and the infusion rate adjusted accordingly, with 10 to 15 μg/mL being therapeutic. Their beneficial effects are attributed to their many potent anti-inflammatory effects on multiple cell types [72,75]. Compared with betamethasone and dexamethasone, neither prednisone nor methylprednisolone contain metabisulfites, and both have shorter half- lives. Although hydrocortisone has the shortest half-life, it has greater mineralocorticoid effect and may cause idiosyncratic bronchospasm in some aspirin-sensitive individuals [76]. For initial treatment of an acute exacerbation of asthma, studies suggest that oral administration of corticosteroids is as effective as intravenous therapy [1,2,77,78]. Therefore, the oral route is preferred unless there is the possibility of impaired gastrointestinal tract transit time or absorption. Inhaled corticosteroids do not have a well-established role for the treatment of acute exacerbations of asthma of hospitalized patients. However, in the Emergency Department setting inhaled, high-dose corticosteroids decrease hospitalization rates for patients not receiving systemic corticosteroids, but their benefit for patients receiving additional, systemic corticosteroids is not established [1,79]. The optimum dosages of corticosteroids for the treatment of acute asthma are also not well established by randomized controlled clinical trials [1,2,80]. One study compared 15, 40, and 125 mg methylprednisolone every 6 hours and suggested that patients improved most rapidly with the 125 mg dose [81]. For example, one study showed no difference between 100 and 500 mg methylprednisolone for the emergency department treatment of asthma [82]. For courses of treatment lasting less than 1 week and for courses lasting up to 10 days, there is no established benefit to slowly tapering the daily oral corticosteroid dose, especially when the patient is also using inhaled corticosteroids [1]. Oxygen Supplemental oxygen therapy should be the initial intervention in the emergency department [1,2]. Because ventilation–perfusion mismatch is the dominant cause of hypoxemia with asthma, the PaO usually2 increases readily in response to low levels (2 to 4 L per minute oxygen by nasal prongs) of supplemental oxygen therapy. Studies have shown that titrated, low-flow oxygen therapy to achieve oxygen saturations of 93% to 95% is associated with better outcomes than the routine use of untitrated, high flow, 100% oxygen therapy [85,86]. In addition to mitigating the cardiac and neurologic complications of severe hypoxemia, low-flow supplemental oxygen minimizes potential episodes of hypoxemia due to the acute administration of β2-adrenergic agonists, decreases elevated pulmonary vascular pressures due to hypoxic vasoconstriction, decreases bronchospasm due to hypoxia, and improves oxygen delivery to respiratory muscles. Fluids No convincing evidence has shown that fluid administration in excess of euvolemia hastens mobilization of inspissated secretions from the airways. Although the data are mixed, inhaled, rather than intravenous, magnesium sulfate may also have a role in the treatment of acute asthma. That is, for severe asthma exacerbations, albuterol nebulized diluted in magnesium sulfate solution may be a more effective bronchodilator than albuterol nebulized in normal saline [88,89]. Because of its lower gas density, some improvement in airway resistance may be achieved by delivering a mixture of helium and oxygen gases to patients with airway obstruction. However, guidelines do not recommend the routine use of heliox for the treatment of asthma and suggest that it be considered only for rare, severe cases unresponsive to standard therapies [1,2]. Some therapeutic agents that are used for the treatment of stable asthma have no established role in the treatment of severe exacerbations of asthma among hospitalized patients.
Amoebae are not generally seen arthritis in dogs back legs uk buy diclofenac gel 20gm with amex, and are only rarely cultured because the parasite concentrates in the walls of the abscess arthritis diet success purchase 20gm diclofenac gel amex. Invasive enterocolitis and hepatic abscess should be treated with oral metronidazole (750 mg every 8 hours for 10 days) or tinidazole (2 g daily early onset arthritis in dogs diclofenac gel 20gm line, divided into three doses, for 3-5 days) (see Table 8. The trophozoite consists of a dorsal convex surface and a flat disk-shaped ventral surface composed of microtubules and microribbons, two nuclei, and four pairs of flagella. Trophozoites adhere to gastrointestinal endothelial cells, disrupt the brush border, cause disaccharidase deficiency, and induce inflammation. All of these mechanisms are thought to account for watery diarrhea and malabsorption. Patients with X-linked agammaglobulinemia have an increased risk of contracting severe prolonged disease, emphasizing the contribution of humoral immunity. Under unfavorable environmental conditions, Giardia can form dormant cysts that are excreted in the stool, and account for spread of disease. Trophozoites attach to gastrointestinal endothelial cells, causing malabsorption and inflammation. Giardia cysts are spread by contaminated water (and sometimes food) and person-to-person contact. A disease of campers (sterilization of water critical for prevention), daycare centers, and sexually active homosexuals. Giardiasis is found throughout the world; it is a common infection in the United States. Giardia cysts are most commonly spread by contaminated water, and multiple waterborne outbreaks have occurred in mountainous regions of the Northeast, Northwest, and Rocky Mountain states, and in British Columbia. Campers must aggressively sterilize drinking water from mountain streams to prevent this common infection. Giardia can also be transmitted from person to person in daycare centers and other confining institutions. This pathogen also has been spread from person to person by sexually active homosexuals. Clinical Manifestations, Diagnosis, and Treatment A patient with this parasite usually has only mild symptoms or is asymptomatic. Adults may complain of abdominal cramps, bloating, diarrhea, anorexia, nausea, and malaise. Chronic disease is less common and results in malabsorption, chronic diarrhea, and weight loss. A diagnosis of giardiasis should be considered in all patients with prolonged diarrhea. Examination of cysts using concentration techniques has a 90% yield after three stool samples. Endoscopy and duodenal biopsy, or duodenal aspiration, are no longer necessary in most cases. Oral metronidazole (250 mg every 8 hours for 5-7 days), tinidazole (2 g as a single dose), or nitazoxanide (500 mg q12h × 3 days) is the treatment of choice (see Table 8. Clinical manifestations are usually mild; the disease is self-limiting, 4- 6 weeks. Diagnosis: a) Stool smear shows no polymorphonuclear leukocytes; cysts are seen in 90% of cases after three stool examinations. Autoinfection can also occur, explaining how ingestion of small numbers of oocysts can cause severe, persistent infection in the immunocompromised host. Cryptosporidium is classified as an intestinal coccidian; it is related to malarial organisms. The mechanisms by which Cryptosporidium causes diarrhea are not completely understood. The pathogen affects intestinal ion transport and causes inflammatory damage to the intestinal microvilli, resulting in malabsorption. This parasite is carried in the intestinal tract of many animals and is also found in water.
Adverse effects Adverse effects of sulfasalazine occur in up to 45% of patients rheumatoid arthritis and gluten cheap diclofenac gel uk, with the majority due to the sulfapyridine component psoriatic arthritis diet coffee buy diclofenac gel on line amex. Serious reactions include hemolytic anemia arthritis in the knee surgery generic diclofenac gel 20gm without prescription, myelosuppression, hepatitis, pneumonitis, nephrotoxicity, fever, rash, and Stevens-Johnson syndrome. Treatment should be discontinued at the first sign of skin rash or hypersensitivity. Sulfasalazine also inhibits intestinal folate absorption, and folate supplementation is recommended with chronic use. The newer mesalamine formulations are well tolerated; headache and dyspepsia are the most common adverse effects. Rarely, acute interstitial nephritis may occur and renal function should be monitored in patients receiving mesalamine. Enteric-release preparations of oral budesonide deliver corticosteroid to a portion of inflamed intestine. This agent has minimal systemic adverse effects due to low bioavailability resulting from extensive first- pass hepatic metabolism. Although systemic exposure is less than other corticosteroids, the use of budesonide in extended maintenance of remission is limited due to concerns with long-term use. Many of these agents have other therapeutic indications such as rheumatoid arthritis (see Chapter 38) or psoriasis (see Chapter 43). These agents are associated with the development of immunogenicity and antidrug antibodies that can result in loss of response in a significant proportion of patients. Use of α-4 integrin inhibitors reduces lymphocyte migration into the intestinal mucosa and inflammation. The most common adverse reactions include headache, arthralgia, nausea, fatigue, and musculoskeletal pain. Common adverse effects include headache, arthralgia, infection, nausea, and nasopharyngitis. Monitoring of complete blood counts and liver function tests is recommended in all patients treated with a thiopurine. Which drug would be most effective to counteract the emesis in this patient without exacerbating her cardiac problem? Although dolasetron is also in this category, its propensity to affect the heart makes it a poor choice for this patient. The antiemetic effect of prochlorperazine, a phenothiazine, is most beneficial against anticancer drugs with moderate to low emetogenic properties. Because of past experiences while traveling, they ask their doctor to prescribe an agent in case they experience diarrhea. Although its effects are not immediate, docusate may be used for mild constipation and is generally considered safe in pregnancy. Castor oil should not be used in pregnancy because of its ability to cause uterine contractions. Mineral oil should not be used in bedridden patients due to the possibility of aspiration. Bismuth subsalicylate compounds may cause a harmless black discoloration of the tongue. She is currently taking several medications, including aspirin, clopidogrel, simvastatin, metoprolol, and lisinopril. Omeprazole may possibly decrease the efficacy of clopidogrel because it inhibits the conversion of clopidogrel to its active form. Misoprostol, a synthetic prostaglandin analog, is contraindicated in pregnancy because it may stimulate uterine contractions. The other medications may be used during pregnancy for the treatment of heartburn (common in pregnancy) or peptic ulcer disease. Results of endoscopy are consistent with moderate Crohn’s disease involving the terminal ileum and proximal large intestine. Delayed-release budesonide is indicated in Crohn’s disease because it releases in the terminal ileum and proximal large bowel and is effective in inducing remission.