
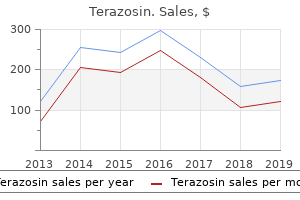
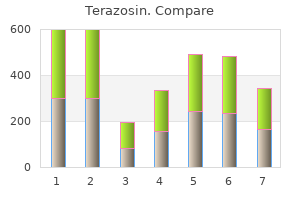
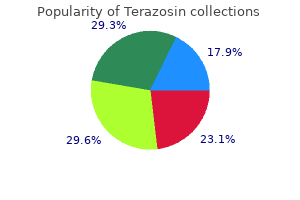
Terazosin
"Order 2 mg terazosin amex, hypertension knee".
By: C. Ressel, MD
Program Director, Florida State University College of Medicine
In American Samoa arrhythmia practice tests cheap terazosin 2 mg free shipping, an out- break of radiculomyeloencephalitis was described in 16 fishermen who had con- sumed raw or undercooked Achatina fulica (giant African snail) blood pressure medication and weight loss generic terazosin 2 mg on-line, an intermediate host of A blood pressure log chart pdf buy generic terazosin 2mg online. In addition to eosinophilia in the spinal fluid and the blood, the disease was characterized by acute abdominal pain, generalized pruritus, and later by pain, weakness, and paresthesia in the legs, and dysfunction of the bladder (urinary retention or incontinence) and the intestine. Half of the patients suffered transitory hypertension or lethargy; three entered a coma and one died. Serologic surveys carried out in Australia, in human populations living in localities where the infection occurs in rats and those living in other places where it does not, indicate that many human infections are asymptomatic. In highly parasitized animals, eggs and larvae may be found in various viscera of the body. No significant differ- ence in weight between parasitized and nonparasitized animals has been confirmed. However, the physical appearance of the animals does not reflect the degree of pathologic changes. For both parasites, the prevalence of the infection is greater in adult than in young rodents, which suggests that rodents do not develop resistance to the infection. Source of Infection and Mode of Transmission: Several species of rodents serve as definitive hosts of A. The cotton rat inhabits areas close to dwellings in both tropical and temperate zones, feeding on both plants and small vertebrate and invertebrate animals, including slugs. All these facts suggest that this rat is a prime reservoir and that it plays an important role in the epidemiology of the parasitosis. Rodents are infected by ingest- ing food or water contaminated with the infective larvae in the mollusk secretions (slime) or by eating the infected mollusks. Man may acquire the infection in the same way, for example, by eating poorly-washed vegetables containing small slugs or their secretions. A study in Guatemala showed that the consumption of mint leaves, alone or as a seasoning in traditional uncooked dishes, correlated directly with the presence of the infection in man (Kramer, 1998). It is believed that children can become infected while playing in areas where slugs are abundant by transferring mollusk secretions found on vegetation to their mouths. An increase in cases in chil- dren occurs in Costa Rica during the rainy season, when slugs are plentiful. Humidity is an important factor in the survival of both the first- and third-stage lar- vae, since they are susceptible to desiccation. These rodents, natural definitive hosts, are infected by consuming mollusks or paratenic hosts that harbor third-stage larvae. The infection rates of mollusks as intermediate hosts are usually high; both the prevalence and the number of larvae an individual mollusk can harbor vary accord- ing to the species. Man, who is an accidental host, is infected by consuming raw mollusks or paratenic hosts such as crustaceans or fish. The ecology of angiostrongyliasis is closely related to the plant community in which the mollusks and rodents live. The frequency of the human parasitosis depends on the abundance of these hosts and the degree to which they are infected, and, also, in the case of A. In places such as Thailand, where infection of the central nervous system caused by Gnathostoma spinigerum has a high prevalence, the two diseases must be differentiated. Although most reports indicate that only in a few cases can the parasite be found in patients’ cerebrospinal fluid or eyes, Hwang and Chen (1991) reported having recovered it by lumbar puncture in 41. Serologic tests are useful for con- firming the presumptive diagnosis (Legrand and Angibaud, 1998). Control: While human angiostrongyliasis is not very prevalent, except in a few areas of high endemicity, prophylaxis is important because there is no known ther- apeutic treatment for the infection. Theoretically, angiostrongyliasis could be con- trolled by reducing rodent and mollusk populations, though practical application seems doubtful. Preventive measures for individuals consist of thoroughly washing vegetables, and hands after garden or field work; not eating raw or undercooked mollusks and crustaceans; and not drinking water that may be unhygienic. Incubation in saturated sodium chloride or in commercial vinegar reduced the number of larvae but failed to prevent the infection in mice (Zanini and Graeff-Theixeira, 1995). Seroepidemiology of abdominal angiostrongyliasis: The standardization of an immunoenzy- matic assay and prevalence of antibodies in two localities in southern Brazil. Eosinophilic radiculomyeloencephalitis: An angiostrongyliasis outbreak in American Samoa related to ingestion of Achatina fulica snails.
In the the theory that addiction involves a dysregulation in the motive pursuit of reward hypertension diabetes purchase terazosin us, the receptors that naturally mediate reward circuitry arrhythmia hereditary order generic terazosin pills, and the repetitive use of addictive drugs reorganizes become desensitized heart attack 70 blockage buy terazosin 2 mg free shipping, which creates the need for more substances, brain circuitry to establish behaviors characteristic of addiction. The prefrontal cortex, responsible for decision making, gets activated with the amygdala, creating a Learning and Memory connection for craving. This activates a neurotransmitter called Hyman (2005) discusses the role of addictive behaviors in usurp- glutamate, which creates an unpleasant feeling associated with ing the neural mechanisms of learning and memory that normal- craving that can cause the addict to try to reduce this discomfort ly shape survival behaviors related to rewards and predictive cues. If survival is too intimately associated in the addict’s mind with Besides the legal, financial, and psychosocial consequences securing the addictive substance, rewards and predictive cues of addictive behavior, the addict also risks neuronal recircuiting develop around the substance. Chronic substance use results in that results in physiologic cycles of addictive behaviors. Dopamine, a powerful neurotransmitter, can shape stimu- Decision Making lus-reward learning, or the behavioral response to reward-related Addictive behaviors negatively affect decision making, as well. Cueing involves significant associational memories, and Noel, van der Linden, and Bechara (2006) suggest that addic- connectionist brain theory suggests that these associations are tion is an imbalance between the neural system that is reactive wired into the brain. For example, a patient placed in an envi- for signaling pain or pleasure and another neural system that is ronment where he or she previously used a substance may be reflective and controls the reactive system. Enhanced sen- make detrimental decisions and fail to learn from their mistakes, sitivity of pituitary beta-endorphin to ethanol in subjects at high contrary to their pre-injury personality. Both deny they have a problem and appear to ignore the derlying neurobiological basis: Neuroimaging evidence for in- consequences of their actions. A predisposition to addiction: Pharmacokinetics, esize that some people have a weak decision-making mechanism pharmacodynamics, and brain circuitry. American Journal of Psychi- in the brain and that the weakness makes them vulnerable to atry, 160(1), 1–2. Self-preservation and the care ity to make appropriate decisions as the compulsive drive for the of the self—ego instincts reconsidered. Stress, dysregulation of drug reward pathways, and the transition to drug dependence. The neurocogni- tive mechanisms of decision making, impulse control, and loss of progressive deterioration of the ability to freely choose. If appropriately treated, addiction can remain in remission, and nurses who have peer support and monitoring have a greater chance of long-term sobriety than the general population. The recovering addict must begin an exploration into self, cultivate a program of well-being, and maintain a long-term goal of sobriety. The bodies of authority in the nursing profession must understand the disease of addiction and its treatment. This un- derstanding may lead to more options for addicted nurses, greater opportunities for them to heal and return to the profession, and a compassionate approach to peers that is congruent with the values of the nursing profession. Which statement about the reward Understanding the Disease circuitry of the brain is correct? Characteristic withdrawal syndrome for Addiction nervous system responsible for the substance If you reside in the United States and automatic functions, and the limbic areas b. Recurrent substance use in situations in system responsible for automatic which it is physically hazardous Instructions functions and the limbic areas of the d. Which statement about predisposition to automatic functions, and the limbic areas (no charge) addiction is correct? A predisposition is usually enough to complete the print form and mail it to stimulus-reward learning? Addicts rarely seek treatment because of service, or company referred to in this b. Were the methods of presentation (text, symptom of post-acute withdrawal in tables, figures, etc. Was the article useful to you in your addicts is associated with increased c Identify contributing factors for work? Injury to which area in a nonaddicted person results in decision making Rate each of the following items from similar to that of the addicted person? The Lifestyle Heart Trial In a prospective, randomised, controlled trial to We carried out trials in 1977 and 1980 to assess the determine whether comprehensive lifestyle short-term effects of lifestyle changes on coronary heart changes affect coronary atherosclerosis after 1 disease with non-invasive endpoint measures year, 28 patients wereassigned to anexperimental (improvements in cardiac risk factors, functional status, group (low-fat vegetarian diet, stopping smoking, myocardial perfusion,2 and left ventricular function3). When only lesions wererandomly assigned to anexperimental group orto ausual-care greater than 50% stenosed were analysed, the control group. Experimental-group patients were prescribed a average percentage diameter stenosis regressed lifestyle programme that included a low-fat vegetarian diet, from 61·1 to 55·8 in the moderate aerobic exercise, stress management training, stopping (8·8)% (11·0)% and from 61·7 smoking, and group support. Control-group patients were not experimental group progressed asked to make lifestyle changes, although they were free to do so.
Strengths Broad definitions exist of online ‘health consumers’ [50] and ‘health seekers’ [51] blood pressure 50 over 70 purchase terazosin cheap online. Weaknesses Lack of a definition that encapsulates the specific concept of health-seeking behaviour on the web heart attack man buy 2 mg terazosin with mastercard. Models & theories Were there any models blood pressure normal karne ka tarika buy terazosin 2mg otc, theories or frameworks identified in the review? Strengths The literature pertaining to the topic spans a number of disciplines including: communication science, medicine, health promotion, social marketing, psychology and information technology from which theories, models and frameworks could be developed. Weaknesses No such models, theories or frameworks were identified generally or in relation to communicable diseases specifically. Weaknesses The literature shows little uniformity in the methods used to research health consumers’ information- seeking on the internet. Strengths There is descriptive evidence about: • Internet accessibility and usage patterns [52-62]. Quality Although there is no explicit assessment of the quality of the evidence in the review, most of the studies which have been included were subject to peer review prior to their publication. Quality There is little consistency between the subject matter of the research undertaken and the methodologies and terminologies used in relation to internet use by health professionals. Health professionals may recommend credible websites to patients [83] and may provide printed information from websites [73]. Behavioural and other changes • One survey showed that 29% of respondents used online information to decide whether or not to consult a doctor and a percentage of these used the internet in conjunction with a doctor’s appointment [62]. It may also improve patients’ self-efficacy [82] and empowers their decision-making about their health [86]. Weaknesses Communication effects • Health professionals are at risk from information overload [70, 80] and have difficulty filtering and identifying the most credible information [70, 77, 80]. Application What has been applied into practice in the area of health information-seeking behaviour on the web for the prevention and control of communicable diseases? There is little evidence of application in practice or the use of interventions for building on the survey data. Focus There is little focus in the literature on specific health topics in general and communicable diseases in particular. A literature review on health information-seeking behaviour on the web: a health consumer and health professional perspective. The references cited in this matrix table and upcoming tables are listed in Appendix 3. Strengths Conceptualisation of trust and reputation management in the public health communicable disease literature focuses on its strategic function and impact; to date, broad-based theoretical or explanatory conceptualisation is in an emergent phase. Weaknesses Not well understood holistically in communicable disease public health; tendency to narrow concept to specific communication functions and frameworks for planning and action. Models & theories Were there any models, theories or frameworks identified in the review? Tools Did the review identify any tools that facilitate step by step practical application? Strengths A body of case studies and retrospective analysis is beginning to accumulate; 30% of identified literature reported empirically tested evidence. Weaknesses Overall, theory and evidence-informed applications of trust and reputation management for communicable disease health communication has been subject to rather limited research and analysis to date, especially in Europe. Behavioural and other changes Behaviour change to reduce influenza transmission (increased hand washing, surface cleaning, avoidance behaviours etc. Weakness Communication effects Paucity of baseline measures of organisational reputational capital or public trust. Behavioural and other changes Very limited evidence on behavioural and other changes. Application What has been applied into practice in trust and reputation management for the prevention and control of communicable disease? Strengths Focus • Primary research and commentaries addressing the impact of discreet, event-specific communication particularly crisis communication, and to a lesser extent risk communication [97, 99,102, 104-113].
This is followed by symmetrical descending flaccid (weak arteria nutricia buy cheap terazosin 5mg, soft) paralysis what is pulse pressure yahoo order terazosin master card, with generalized weakness and progression to respiratory failure hypertension ppt terazosin 1 mg on-line. Symptoms begin as early as 12-36 hours after inhalation, but may take several days after exposure to low doses of toxin. A bioterrorism attack should be suspected if multiple casualties simultaneously present with progressive descending flaccid paralysis. Toxin is not dermally (skin) active and secondary aerosols are not a hazard from patients. Airway necrosis and pulmonary capillary leak resulting in pulmonary edema would likely occur within 18-24 hours, followed by severe respiratory distress and death from hypoxemia (low blood oxygen) in 36-72 hours. Diagnosis: Acute lung injury in large numbers of geographically clustered patients suggests exposure to aerosolized ricin. The rapid time course to severe symptoms and death would be unusual for infectious agents. Treatment: Management is supportive and should include treatment for pulmonary edema. Gastric lavage and cathartics (emetics) are indicated for ingestion, but charcoal is of little value for large molecules such as ricin. Prophylaxis: There is currently no vaccine or prophylactic antitoxin available for human use. Ricin is non-volatile, and secondary aerosols are not expected to be a danger to health care providers. Patients may also present with nausea, vomiting, and diarrhea if they swallow the toxin. Artificial ventilation might be needed for very severe cases, and attention to fluid management is important. Effects on the airway include nose and throat pain, nasal discharge, itching and sneezing, cough, shortness of breath, wheezing, chest pain and bloody sputum. Severe intoxication results in prostration, weakness, ataxia, collapse, shock, and death. Diagnosis: Should be suspected if an aerosol attack occurs in the form of "yellow rain" with droplets of variously pigmented oily fluids contaminating clothes and the environment. Soap and water washing, even 4-6 hours after exposure can significantly reduce dermal toxicity; washing within 1 hour may prevent toxicity entirely. Prophylaxis: The only defense is to prevent exposure by wearing a protective mask and clothing (or topical skin protectant) during an attack. Isolation and Decontamination: Outer clothing should be removed and exposed skin decontaminated with soap and water. Secondary aerosols are not a hazard; however, contact with contaminated skin and clothing can produce secondary dermal exposures. Environmental decontamination requires the use of a hypochlorite solution under alkaline conditions such as 1% sodium hypochlorite and 0. However, the general principles outlined within this chapter hold true regardless of the agent used. Refer to the guidelines in the bioagent section above for a generic approach to assessment. Additionally, decontamination procedures for chemical agents are analogous to the procedures followed for a suspected biological agent. Exposure may cause skin burns and necrosis, eye burns with ulceration and possible perforation, airway disease with shortness of breath, wheezing, and chest pain and suppression of the immune system. Severe intoxication results in prostration, weakness, seizures, collapse, shock, and death. Diagnosis: Should be suspected if an aerosol attack occurs in the form of a vapor with symptoms as outlined above or contact with an oily yellow to brownish liquid is encountered. Treatment: Skin: Soothing creams to burns, analgesics, antibiotics to treat/prevent infection. Eyes: Soothing eye drops, topical mydriatics, topical antibiotics, and sunglasses. Prophylaxis: The only defense is to prevent exposure by wearing a protective mask and clothing (or topical skin protectant) during an attack.
Purchase terazosin in united states online. CRC Practice Exam Questions | CRC Practice Exam Layout.