
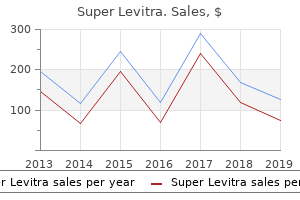
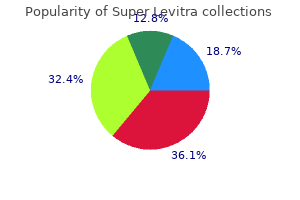
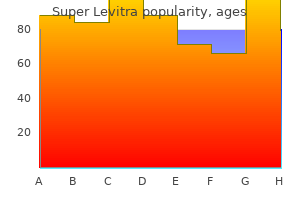
Super Levitra
"Buy super levitra 80 mg amex, erectile dysfunction juice drink".
By: O. Luca, M.A., M.D.
Co-Director, University of Colorado School of Medicine
This must include the opportunity to meet the surgeon or interventionist who will be undertaking the procedure erectile dysfunction treatment options purchase 80mg super levitra fast delivery. H20(L2) Patients must be given an opportunity to discuss planned surgery or interventions prior to planned Immediate dates of admission erectile dysfunction at age 24 80 mg super levitra overnight delivery. Section H – Communication with patients Implementation Standard Adult timescale consequences of their decisions so that they are able to give informed consent erectile dysfunction natural treatment reviews purchase 80mg super levitra with mastercard. H22(L2) Patients and their partner, family or carers must be given details of available local and national Immediate support groups at the earliest opportunity. H23(L2) Patients must be provided with information on how to claim travel expenses and how to access Immediate social care benefits and support. H24(L2) A Practitioner Psychologist experienced in the care of congenital cardiac patients must be available Within 1 year to support patients at any stage in their care but particularly at the stage of diagnosis, decision making around care and lifecycle transitions, including transition to adult care. H25(L2) When patients experience an adverse outcome from treatment or care the medical and nursing staff Immediate must maintain open and honest communication with the patient and their family. Identification of a lead doctor and nurse (as agreed by the patient or their family) will ensure continuity and consistency of information. A clear plan of ongoing treatment, including the seeking of a second opinion, must be discussed so that their views on future care can be included in the pathway. An ongoing opportunity for the patient to discuss concerns about treatment must be offered. Section I - Transition Implementation Standard Adult timescale I1(L2) Congenital Heart Networks must demonstrate arrangements to minimise loss of patients to follow-up Within 1 year during transition and transfer. The transition to adult services will be tailored to reflect individual circumstances, taking into account any special needs. I2(L2) All services that comprise the local Congenital Heart Network must have appropriate arrangements Immediate in place to ensure a seamless pathway of care, led jointly by paediatric and adult congenital cardiologists. I3(L2) There will not be a fixed age of transition from children’s to adult services but the process of Immediate transition must be initiated no later than 12 years of age, taking into account individual circumstances and special needs. Clear care plans/transition passports must be agreed for future management in a clearly specified setting, unless the patient’s care plan indicates that they do not require long-term follow-up. I5(L2) Patients, partners, families and carers must be fully involved and supported in discussions around Immediate the clinical issues in accordance with the patient’s wishes. The views, opinions and feelings of the patient must be fully heard and considered, and the patient must be offered the opportunity to discuss matters in private, away from their parents/carers if they wish. I6(L2) All patients transferring between services will be accompanied by high quality information, including Immediate the transfer of medical records, imaging results and the care plan. Section I - Transition Implementation Standard Adult timescale I7(L2) Young people undergoing transition must be supported by age-appropriate information and lifestyle Immediate advice. Management of young people arriving in the adult service will aim to ensure that they are fully confident in managing their own condition and health care. The Cardiologist will discuss the treatment plan with the young person and discuss it with their family/carers when appropriate. I8(L2) The particular needs of young people with learning disabilities and their parents/carers must be Immediate considered, and reflected in an individual tailored transition plan. I9(L2) Young people must have the opportunity to be seen by a Practitioner Psychologist on their own. Immediate Psychological support must also be offered to partners/family or carers. J2(L2) All female patients of childbearing age must have access to a service that provides specialist Immediate advice on contraception and childbearing potential and counselling by practitioners with expertise in congenital heart disease. Written advice about sexual and reproductive health, and safe forms of contraception specific to their condition must be provided. They must have ready access to appropriate contraception, emergency contraception and termination of pregnancy. The principle of planned future pregnancy, as opposed to unplanned and untimely pregnancy, should be supported. J3(L2) Specialist genetic counselling must be available for those with heritable conditions that have a Immediate clear genetic basis. J5(L2) Patients must be offered access to a Practitioner Psychologist, as appropriate, throughout family Immediate planning and pregnancy and when there are difficulties with decision-making, coping or the patient and their partner are concerned about attachment. Section J – Pregnancy and contraception Implementation Standard Adult timescale pregnancy in congenital heart disease, with arrangements for appropriate cover within the centre. J7(L2) Patients actively considering pregnancy, for whom pregnancy may carry a moderate or high Immediate (class 2-4) risk, must receive joint pre-pregnancy counselling with the cardiologist and a maternal medicine specialist (Consultant Obstetrician) with expertise in pregnancy in women with congenital heart disease.
Positive test:Aw heal>2m m in m ean diam eter to anypenicillin reag ent;erythem a m ustbe present erectile dysfunction drug warnings buy generic super levitra 80mg line. Apositive historyand a positive skin testg ives a 50% chance of an im m ediate reaction if penicillin is g iven (J Allerg yClin Im m unol1998;101:S465 erectile dysfunction underwear purchase generic super levitra canada. Aneg ative testto m ajorand m inor determ inants g ives a 97–99% probabilityof no im m ediate reaction if penicillin is g iven (J Allerg yClin Im m unol1998;101:S465 erectile dysfunction protocol secret purchase super levitra us. E picutaneous test Histam ine Diluent Conclusion N eg Pos N eg D o epiderm altest;w heal2m m larg er than orig inalw healat15–20m in is positive N eg Neg N eg False neg ative. Experience with cephalosporins Literature review of 15,987patients w ho received firstor second g eneration cephalosporins show ed reactions in 8. Areview of 9388patients w ith a historyof penicillin allerg yshow ed 2cases of anaphylaxis (0. The rate of cephalosporin reactions w ith a positive penicillin skin testis 6/135(4. Patients w ith an allerg ic reaction to a cephalosporin should notreceive the sam e ag entag ain,butother cephalosporins w ith differentside chains m aynotcause cross reactions. Anim alstudies sug g estside-chain specific antibodies m aydom inate the im m une response to cephalo sporins (Biochem 1971;123:183. This testing detects 90–97% of allerg ic patients; because lack of m inordeterm inants m isses 3–10% of allerg ic patients,caution is necessary. Patients athig h risk of anaphylaxis (historyof penicillin-induced anaphylaxis,urticaria,asthm a etc should be tested w ith a 100-fold dilution of testreag ents before testing fullstreng th. A10-fold dilution is sug g ested forothertypes of im m ediate,g eneralized reactions w ithin the pastyear. Testm ethods are described above using the epicutaneous (scratch)testfollow ed bythe intraderm altest. Penicillin desensitization should be perform ed in a hospitalbecause Ig E -m ediated reactions can occur,althoug h theyare rare. Manag em entof Allerg ic Reactions M edicalfacilities should have a protocolfordealing w ith allerg ic reactions,especiallyanaphylaxis. Epinephrine:Ig E -m ediated reactions Antihistam ines:Accelerated and late urticaria,m aculopapular rashes Glucocorticoids:Severe urticaria,prolong ed system ic anaphylaxis,serum sick-ness,contactderm atitis,exfoliative and bullous skin reactions, interstitialnephritis,pulm onaryand hepatic reactions 7. Probenecid increases levels of acetam inophen,acyclovir, am inosalicylic acid,barbiturates,beta-lactam antibiotics,benzodiazepines,bum etanide, clofibrate,m ethotrexate,furosem ide,and theophylline Ciprofloxacin (see fluoroquinolones) Clarithrom ycin Carbam azepine* Increased carbam azepine levels and possible reduction in clarithrom ycin effect(Ann Pharm acother 28:1197,1994)—avoid Cisapride* Ventricular arrhythm ias—avoid Disopyram ide* Increased disopyram ide levels w ith cardiac arrhythm ia (L ancet349:326,1997)—avoid Pim ozide Increased pim ozide levels w ith cardiac toxicity(Clin Pharm acolTher 59:189,1996) R ifabutin Increased rifabutin levels w ith uveitis (G enitourin M ed 72:419,1996) Seldane* Ventricular arrhythm ias—avoid Theophylline E levated theophylline levels Clindam ycin Antiperistaltic ag ents Increased risk and severityof C. Voriconazole inhibits cytochrom e P-450 enzym es) Astem izole* R isk ventricular arrhythm ia—avoid Barbiturates Increase barbiturate levels—avoid long acting barbiturates Benzodiazepines Anticipated prolong ed sedative effect—avoid m idazolam ,triazolam ,and alprazolam Calcium channelblockers M ayincrease calcium channelblocker level—m onitor for toxicity Cisapride* R isk ventricular arrhythm ias—avoid Cyclosporine R isk nephrotoxicity—use half cyclosporine dose and m onitor levels E rg ot R isk erg otism Pim ozide* R isk ventricular arrhythm ias—avoid Q uinidine* R isk ventricular arrhythm ias—avoid R ifam pin* R educe voriconazole levels—avoid R ifabutin* R educe voriconazole levels—avoid Sirolim us R isk sirolim us toxicity—avoid Statins Anticipated increase in statin levels—consider low er statin dose Tacrolim us Increase tacrolim us levels—reduce dose to 1/3 and m onitor W arfarin Increase prothrom bin tim e 2×—m onitor prothrom bin tim e * ConcurrenThise should be avoided if possible. Title: 2004 PocketBook of I nfectious Disease Therapy,12th E dition Copyrig ht©2004L ippincottW illiam s & W ilkins > Table of Contents > Preventive Treatm ent> AdultIm m unization Schedule AdultI m m unization Schedule A. Vaccine 19–49 yrs 50–64 yrs >65 yrs Tetanus,diphtheria Booster dose every10yrs Influenza M edical,occupational,or household contact Annualdose indication Pneum ovax M edicalindication 1dose or revaccination at5yrs M easles,rubella,M um ps 1dose if hx unreliable Varicella 2doses (0and 4–8w ks)if susceptible Hepatitis A 2doses (0,6–12m o)for indications Hepatitis B 3doses (0,4,and 6m o)for indications N ote:The onlytrue contraindications to vaccinations are a historyof severe allerg ic reaction after a prior dose or a vaccine constituent. Travelers to epidem ic area po × 4qod,boosters at5-yr intervals Typhim Vi capsular polysaccharide vaccine. W om en ex posed during first20w k should have rubella serolog yand if notim m une should be offered abortion. Cholera N otrecom m ended because risk is low and vaccine has lim ited effectiveness (L ancet1990;1:270) Typhoid fever Recom m ended for travelto ruralareas of countries w here typhoid fever is endem ic or anyarea of an outbreak,prim arilytravelers outside the usualtouristroutes in L atin Am erica,Asia,and Africa L ive oralvaccine—Vivotif (1cap everyother day× 4starting atleast2w k before travel)—is preferred over the parenteralkilled bacterialvaccine because of com parable efficacy,long er protection,and better tolerance (L ancet1990;336:891);available from Berna Prod (800-533-5899). A booster is recom m ended at6–12m o,buta sing le dose is considered adequate protection if g iven atleast2–4 w k before travel. Tw inrix requires tw o doses separated by1m onth prior to travel,otherw ise the m onovalentvaccine is preferred. M ajor risk areas are China,K orea,allof Africa,M iddle E ast,Southern and Pacific Islands,Am azon reg ion of South Am erica,Haiti,D om inican Republic,and SoutheastAsia (M ed L etter 2001;43:67). Adults w ho have notreceived atleastthree doses of Td should com plete prim ary series. Persons are considered im m une to rubella if theyhave a record of vaccination after their firstbirthdayor laboratoryevidence of im m unity.
This book is dedicated to the loving memory of my parents erectile dysfunction obesity purchase 80 mg super levitra visa, Kazem and Badri-Zaman Khatami erectile dysfunction heart disease diabetes cheap 80mg super levitra fast delivery. The invaluable support and encouragement of the following individuals is also acknowledged with great appreciation: John H erectile dysfunction causes and solutions super levitra 80mg otc. D, mentor/friend and senior colleague at the University of Pennsylvania, who instilled the love of science and devotion to serve the public in me and who shaped my early career and initially trained me in immunobiology of inflammatory diseases that resulted in our ‘accidental’ discoveries in 1980’s that are suggestive of the first evidence for a direct association between inflammation and tumorigenesis; Edward J. The Editor also wishes to pay tribute to the memory of her good friend, Shirin (Shirley) Mirsepassi- Toloui, M. Introduction Rudolph Virchow, in the 19th century noted that “the signs of inflammation are four; redness, and swelling, with heat & pain“. Since this historical observation, the role of inflammation in the genesis and progression of many acute diseases (e. However, the mechanisms of inflammatory responses in the induction of a wide range of inflammatory diseases or cancer that are manifested in tissues as site- specific conditions are not understood. For example, the ongoing debates and controversies in literature whether inflammation is protective in preventing carcinogenesis or it is a cause of cancer demonstrate lack of understanding in differentiating the role of acute and chronic inflammatory responses in preventing or inducing cancer. Consequently, despite heavy public investment for over four decades on cancer war, too many expensive and out-of- focus clinical trials that use potent drugs which are pro-inflammatory mediators or inhibitors of growth factors (poisons) have caused serious and life-threatening side-effects for cancer patients (reviewed in Khatami 2011 a, b). This chapter will provide a brief overview of recent definitions for acute and chronic inflammation and the role that inflammation plays in the induction of acute and age- associated chronic diseases, with emphasis on cancer. Attempts were made to demonstrate that self-terminating natural property of immune system (immune surveillance) in acute inflammation is protective to the body (‘Friend’). However, unresolved and persistent inflammation (oxidative stress) could change the dynamics of immune responses creating an immunological chaos or ‘immune tsunami’ that would cause loss of architectural integrity and function in susceptible tissues leading to initiation, progression and manifestation of a wide range of chronic conditions or cancer (‘Foe’) that are very likely interrelated and potentially preventable (Khatami, 2008, 2009, 2011 a, b). Outlines of a framework for future designs of clinical trials based on a concept that Inflammation, Chronic Diseases and Cancer – 4 Cell and Molecular Biology, Immunology and Clinical Bases inflammation is a common denominator in the genesis and manifestation of a wide range of age-associated chronic diseases and cancer will also be presented. Acute inflammation: Protective, self-terminating property of immune system: Body’s immune surveillance During evolutionary process, inflammation became an inherent protective and self- limiting property of immune system to guard the body against harmful elements that the body recognizes as foreign elements (stimuli or irritants). Briefly, effective immunity is provided through natural pleiotropy or duality (polarity) of immune cells via acute inflammation to facilitate the organ systems the ability to return to normal physiological function after encountering internal or external foreign elements [e. Acute inflammatory process was recently defined as the balance between two highly regulated and biologically opposing arms termed ‘Yin’ (apoptosis, growth-arresting, pro- inflammatory or tumoricidal) and ‘Yang’ (wound healing, growth-promoting, anti- inflammatory, tumorigenic) responses of immune cells with intimate participation of vasculature (Khatami, 2008) (Figure 1). The principal mission of acute inflammation (immune surveillance) is two folds: 1. Encounter (sense), process/digest, destroy and eliminate intrinsic or extrinsic foreign elements and infected/injured host tissue, 2. Resolve and terminate inflammation and repair and construct or remodel the target/injured host tissue. The major outcome of an acute inflammation is lymphocyte-derived clonal expansion, increased synthesis of allergen- or pathogen-specific antibodies and plasma and memory T and B cells (Khatami 2008, 2009, 2011 a, b). Simply described, apoptosis (‘Yin’) is responsible for production of death signals and oxidants to destroy the enemy and injured host cells, while wound healing (‘Yang’) is required to counteract apoptosis and neutralize and remove the toxic ‘debris’ from the ‘battle field’ and to reconstruct and repair the host and resolve or terminate inflammation. Stimuli- (stressor-) induced a well balanced signals between 2 biologically opposing arms, ‘Yin’ (growth- arresting) and ‘Yang’ (growth-promoting) processes through elaborate cross-talks between immune and non-immune systems (e. The host defense system has also tolerance and remembrance capacities to develop memory and regulatory T or B cells when encountering specific foreign elements including cancerous cells (Khatami 2005 a, 2007, 2008, 2009, 2011 a). These events include simultaneous expression of anti-inflammatory mediators, hormones and growth factors (e. These interdependent and complex immunobiological cross talks are examples of numerous other sophisticated bilateral communications between immune and non-immune systems that are orchestrated during acute inflammatory responses to maintain and protect the psychophysiological and architectural integrity of organ systems throughout life. Acute inflammation induces bilateral and balanced responses between apoptotic (‘Yin’) and wound healing (‘Yang’) pathways. Pleiotropic roles of immune responses and oxidative stress-induced immune suppression. Unresolved inflammation: ‘Immune tsunami’ and loss of architectural integrity in immune-responsive and immune-privileged tissues Unresolved inflammation was defined as the loss of balance between ‘Yin’ and ‘Yang’ of acute inflammation. Briefly, acute inflammation provides immunity (immune surveillance) and protection of target tissues via two major mechanisms (reviewed in Khatami 2009, 2011 a): a. Immune-responsive tissues, the sites of initial contact and processing of internal or external stimuli include squamous and grandular epithelial tissues, epithelial-associated mucosal surfaces (e. Immune surveillance in the immune- privileged tissues (self tolerance or ignorance) is provided by presence of one or a combination of barriers [e. Inflammation and aging could create immune dysfunction (immune tsunami) that cause signal switches by inducing local immune-responsiveness in tissues that are naturally immune-privileged causing tissue necrosis and neurodegenerative disorders.
Find out how to tell if your baby has asthma and what you can do to treat or prevent it erectile dysfunction underlying causes buy super levitra with american express. Learn how to know if your baby might be allergic to your cat erectile dysfunction treatment south florida purchase 80 mg super levitra fast delivery, dog erectile dysfunction caused by radiation therapy buy super levitra with visa, or other pet. Allergy and Asthma Foundation of America. American Academy of Allergy Asthma and Immunology. What can I do to prevent my child from getting allergies in the first place? If your child is allergic to a pet, the only foolproof solution is to give the animal away. But children are usually exposed to the most dust mites in the bedroom, where mattresses and pillows are veritable dust-mite condominiums. "Keep in mind that testing tells you what your child is allergic to at that point, but it may change as your child gets older," says Seattle pediatric allergist Frank S. Virant. So if the blood test does suggest an allergy, the next step for your little sniffler may be a skin test. Pollen-related allergies are more common in spring, summer, and fall. How can I figure out what my child is allergic to? Each allergic person has a threshold that must be reached before an allergen causes a reaction, and this can take several months. If my child is allergic, when will I know? Kids with nasal allergies are also more prone to ear infections , asthma , and sinus infections. Because the symptoms of nasal allergies are much like cold symptoms - runny nose, watery eyes, cough, nasal congestion, sneezing - it can be tough to tell the difference. 10 signs that your child has allergies, not a cold. Nearly 85 percent of allergy sufferers are allergic to dust mites. How common are allergies in kids? These chemicals irritate the body and cause symptoms such as a runny nose, sneezing, itching, and coughing Symptoms can be mild or more severe, intermittent (seasonal, for example), or ongoing because of constant exposure to the allergen. When a child with allergies comes into contact with an allergen - either by touching it, breathing it, eating it, or having it injected - her body mistakenly views it as a dangerous invader and releases histamines and other chemicals to fight it off. An allergy is an immune reaction to a substance in the environment called an allergen. If exercise is the only asthma trigger, a medication that the child takes prior to exercising to prevent the airways from constricting may be prescribed, but usually exercise induced asthma is a sign of poorly controlled asthma. However, one-third of these who were asthma free at puberty have asthma symptoms in their mid- twenties. Steroids treat inflammation in the lungs, preventing asthma attacks and reducing symptoms. Again, if the child responds well to a trial of asthma medications, this is also indicative of asthma. Q. How can the doctor know it is asthma when she is only two months old? Even after the cold is gone, asthma symptoms along with airway swelling can last for several weeks. If the symptoms repeatedly improve it is likely asthma and a treatment plan can be followed to keep the infant well controlled. A. Children are put on puffers when the physician has reason to believe their airways are inflamed and or congested. Q. My baby is wheezing and was put on puffers; does that mean she has asthma?
Aminosalicylates for Ulcerative Colitis Efficacy for Induction and Maintenance of Remission Due to favorable efficacy and safety profiles erectile dysfunction doctor dallas purchase cheap super levitra, oral aminosalicylates remain the stan- dard treatment for mild to moderate extensive ulcerative colitis erectile dysfunction age range 80mg super levitra free shipping. For the remission of active ulcerative colitis erectile dysfunction protocol free buy online super levitra, aminosalicylates were evaluated in a 2006 Cochrane meta-analysis of 21 studies (9 placebo-controlled) incorporating over 2,100 patients [40]. A sta- tistically insignificant trend for superiority of mesalamine over sulfasalazine for endoscopic and clinical improvement was observed. Thus, any of the oral aminosalicylate formulations may be a reasonable choice for the initial treatment of mild to moder- ate extensive colitis. For left-sided disease, including sigmoiditis and proctitis, rectally administered treatments have had the most success in inducing remission. Randomized clinical trials have shown local topical treatments with foams, enemas, or suppositories are more effective than oral medications at inducing and maintaining remission, and a combination of oral medications and local therapy is more effective than oral therapy alone [41]. More recently, even patients with extensive ulcerative colitis were shown to have increased benefit when a local therapy was added to an oral regimen [42]. Like that done for the induction of remission, a Cochrane analysis completed in 2006 evaluated aminosalicylates for the maintenance of remission. Sulfasalazine showed a slight but statistically significant benefit over mesalamine in maintaining remission. While there was no difference in adverse effects or with- drawal due to side effects, many of the analyzed trials excluded patients intolerant to sulfasalazine, thereby incorporating an inherent bias. In summary, for mild to moderate exten- sive ulcerative colitis, aminosalicylates are effective for both induction and mainte- nance of remission. There appears to be little, if any, proven difference in clinical efficacy between sulfasalazine and other mesalamine agents. Sulfasalazine doses between 2 and 4 g have been recommended for active and qui- escent disease though dose-dependent side effects are more common at doses higher than 2 g/day [20]. Higher dosing for more active disease is conceptually more appealing because presumably higher mucosal concentrations of drug are more effective given the improved outcomes observed with the addition of local therapies to oral regimens. Moreover, Cochrane analyses have indicated a trend toward a dose–response relationship [40]. However, evidence for higher doses to achieve or maintain remission has been inconsistent and the question of whether mesalamine doses above 4 g/day might benefit certain subgroups remains unanswered. Despite some evidence of improved dose-related outcomes when partial response or clinical improvement is used as an endpoint, multiple clinical trials have shown no benefit to doses of mesalamine above 2. However, data from subgroup analyses of patients with more refractory disease indicate a possible added benefit with higher doses. Therefore, there may be a steroid sparing role for higher doses of mesalamine, though this hypothesis has yet to be tested. Unfortunately, owing to the variability of end points and definitions of response and remission used in clinical trials, using the available literature for direct comparison of the efficacy of different formulations of aminosalicylates is problematic [46]. This methodologic variability can produce widely differing results depending on which definitions and end points are used. However, one clear difference between formulations is the required dosing schedule and pill burden. While studies have not been designed to determine if the multimatrix release system is superior to other mesalamine formulations in ulcerative colitis, it appears to be at least equivalent. A once-daily dosage of granulated mesalamine (Apriso™) was shown to be effective in doses up to 3. Sixty-five percent of respondents reported missed medications, and approximately 30% reported missing medications at least once per week [49]. Some epidemiologic data have demonstrated an increased incidence of colon cancer with a longer duration of disease [52]. The extent and severity of inflammation also are important factors contributing to the risk of cancer [53]. Mesalamine is believed to have a possible chemo- protective effect due to its anti-inflammatory properties and possibly other unique properties that may disrupt molecular pathways in the pathogenesis of colon cancer [57]. Large prospective, placebo-controlled studies are unlikely to be forthcoming because of sheer impracticality and large numbers of patients and follow-up required. Siegel commonly used for the treatment of Crohn’s disease, the data supporting the use of aminosalicylates in these patients are scant, and expert opinions have gradually excluded them from treatment algorithms. The most recent exciting developments regarding aminosalicylates have resulted in easier-to-tolerate formulations with a lower pill burden. Ideally, future research will teach us which subgroups will benefit the most from these therapies.
Order discount super levitra. 10 Testosterone Killers | Habits And Foods That Decrease T Levels.