
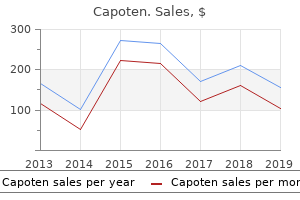
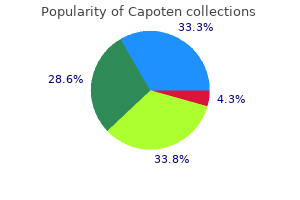
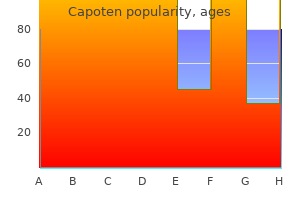
Capoten
"Buy discount capoten 25 mg on line, medications 247".
By: O. Rathgar, M.A., Ph.D.
Co-Director, David Geffen School of Medicine at UCLA
It then decreased abruptly at the triceps surae tension must be overcome by extrinsic end of the stance phase to disappear more or less forces if the body is to be brought forward medications such as seasonale are designed to buy 25mg capoten amex. The heterony- most of the stance phase medications starting with p purchase capoten with american express, triceps surae undergoes a mousfacilitationhadasimilartimecourse schedule 8 medications list generic 25mg capoten with mastercard,probably lengthening contraction, known to evoke strong Ia reflecting modulation of the presynaptic inhibition discharges. Increased presynaptic inhibition of the Studies in patients 367 homonymous Ia excitatory feedback, together with stretch reflex. In this respect (i) pre- synaptic inhibition of gastrocnemius-soleus Ia affer- Running ents has been shown to produce a large decrease Increased presynaptic inhibition of soleus Ia in gastrocnemius medialis-induced non-reciprocal terminals group I inhibition of soleus motoneurones (Rossi, Decchi & Ginanneschi, 1999), and (ii) Ia excitation During the stance phase of running the H reflex has canbeopposedbynon-reciprocalgroupIinhibition, been reported to be smaller than during walking especially during strong contractions (Marchand- (Capaday & Stein, 1987), or of the same amplitude Pauvert et al. It is therefore conceivable, when the H reflex amplitude is expressed as a per- though counter-intuitive, that depression of the Ia centage of Mmax, which varies throughout the gait input to interneurones mediating non-reciprocal cycle(Simonsen&Dyhre-Poulsen,1999). Eitherway, group I inhibition is required to maintain the con- given the much higher level of EMG activity during tribution of the soleus stretch reflex to the pushing running, there is evidence for an increase in pre- off of the foot. Studies in patients and clinical implications Functional significance Capaday & Stein (1987) suggested that the increased Methodology presynaptic inhibition would reduce the gain of the stretchreflextominimisethepotentialforinstability the different techniques reviewed on pp. This view was challenged by Simon- with various central nervous system (CNS) lesions. In any case, presynaptic inhibition may have only weak In clinical studies on patients, simple methods are depressive effects on the reflex responses to abrupt preferable. A somewhat paradoxical explanation the first shock of the train and the test stimulation). Suppression of the H reflex by brief vibra- Iles & Roberts, 1986;Koelman et al. These two factors are activity-dependent heteronymous vibratory inhibition (Butchart et al. Because these changes are in the same direc- accentuated by the fact that post-activation depres- tion, they cannot be due to a change in presynap- sion is decreased in spastic patients (see Chapter 2, tic inhibition of Ia terminals (cf. In addition, the finding that presynaptic reflectadecreaseinthenumberofIaafferentsand/or inhibition of Ia terminals with PAD has only a small in their conduction velocities. Whatever their ori- effect on the reflex responses to abrupt stretch (cf. However, decreased presynaptic inhi- bition of Ia afferents with PAD does exist in some spastic patients and contributes to their stiff gait, and it may be clinically useful to evaluate its extent Spasticity because there are drugs which act mainly on this mechanism. Over-interpretation of decreased presynaptic inhibition In the 1970s–1990s, it was popularly held that a Changes in presynaptic inhibition in patients decrease in presynaptic inhibition of Ia terminals with hemiplegia after stroke was one of the spinal mechanisms, perhaps even Lower limb the main mechanism, underlying the stretch reflex exaggeration characterising spasticity. Intellectually In contrast to the many investigations which relied satisfying at the time, this view was based on what is on homonymous vibratory inhibition of the soleus now known to be a flawed technique: the depression Hreflex (an inappropriate technique, see above), of the soleus H reflex by prolonged homonymous the results obtained with two independent and reli- vibration on the Achilles tendon. It was postulated able methods show that there is no change in pre- and for long accepted that the mechanism underly- synaptic inhibition of Ia terminals in the lower limb ing this reflex suppression is presynaptic inhibition of patients with hemiplegic spasticity. Because this reflex amount of femoral-induced heteronymous facilita- suppression is decreased in most spastic patients, it tion of the soleus H reflex is similar on the affected becamegenerallyacceptedthattherewasadecrease side of hemiplegic patients and in age-matched nor- in presynaptic inhibition of Ia terminals with PAD mal subjects. Sim- in these patients (Delwaide, 1973, 1993;Delwaide & ilarly, presynaptic inhibition of homonymous soleus Pennisi, 1994;Burke & Ashby, 1972; Ashby, Verrier & Ia terminals, as assessed with D1 inhibition of the Carleton, 1980;Taylor, Ashby & Verrier, 1984; soleus H reflex, was found to be symmetrical on the Studies in patients 369 affected and unaffected sides of hemiplegic patients 15 after stroke, and of much the same magnitude as in (b) normal subjects (Aymard et al. No correlation has been found between the severity of spasticity and the reduction in D1 inhibition. The reduction in the D1 inhibition of the FCR H reflex suggests that presynaptic inhibition of FCR Ia ter- 0 minals is depressed on the affected side in patients Controls Para Hemi with hemiplegia. Changes in presynaptic inhibition of femoral Ia terminals to although to a lesser extent, on the unaffected side soleus in spastic patients. The amount of heteronymous facilitation of of stroke patients (Aymard et al. Each horizontal bar represents one subject and the hatched terminals in patients with spinal cord lesions columns show the mean and 1 SEM in the three populations. Modified In contrast with results obtained in the lower limb of from Faist et al. If the corticospinal control was normally exerted exaggerated on the affected side of most hemiplegic tonically, corticospinal lesions would be expected patients, there was no evidence for decreased pre- to produce a decrease in presynaptic inhibition of synaptic inhibition of Ia terminals on soleus, even in Ia terminals on FCR and an increase in presynaptic patients with a lesion in the territory of the anterior inhibition of Ia terminals on soleus. This would hemiplegia in the absence of any other evidence to imply that the organisation of the cortical control of suggest spasticity or motor impairment. However, this view is not supported by evidence from parkinsonian patients (p. A decrease in presynaptic inhibition of Ia terminals may not be responsible for the stretch reflex exag- geration which characterises spasticity measured at Spinal cord lesions rest,butthelackofcontrolofPADinterneuronesdur- Whatever the lesion in the spinal cord, presynap- ing motor tasks could still contribute to the motor tic inhibition is decreased on Ia terminals of the disability of these patients. This cannot be due to the interruption during both voluntary movement and gait.
The most common design type is over the needle; the needle • Use veins with a large blood volume flowing through them is used to start the IV treatment 5th metatarsal stress fracture purchase 25mg capoten fast delivery, then it is removed medicine park oklahoma best order for capoten. Many drugs cause irritation and phlebitis in catheter to start an IV medicine reaction buy genuine capoten online, one that is much smaller than the small veins. Reasons include the difficulty of sta- patient, drug, dosage, date, time of mixing, expiration date, bilizing and maintaining an IV line at these sites. The of several IV set-ups, including a scalp–vein needle and tubing, risks of serious or fatal complications are too high. When it is necessary to change and functioning properly (eg, catheter not clotted, IV fluid not an IV site, use the opposite arm if possible. If leak- Drug Preparation age occurs, some drugs are very irritating to subcutaneous tis- Most IV drugs are prepared for administration in pharmacies and sues and may cause tissue necrosis. When a nurse must prepare a medication, • Maintain sterility of all IV fluids, tubings, injection sites, drug considerations include the following. Other formulations contain various substances that the bloodstream, breaks in sterile technique can lead to serious are not sterile, pure enough, or soluble enough to be in- systemic infections (septicemia) and death. In recent years, there have been • When two or more medications are to be given one after the numerous reports of medication errors resulting from IV other, flush the IV tubing and catheter (with the infusing IV fluid administration of drug preparations intended for oral use!! After irriga- should have a blunt tip that will not connect to or penetrate tion, heparin then needs to be reinstilled. Most drugs given by IV push (direct diluted prior to IV administration and powdered medications injection) can be given over 2–5 minutes and most drugs diluted must be reconstituted appropriately (eg, the correct amount in 50–100 mL of IV fluid can be infused in 30–60 minutes. In addition, be sure potassium or magnesium), be sure the medications are compati- any reconstituted drug is completely dissolved to avoid par- ble with the other substances. Consult compatibility charts (usu- ticles that may be injected into the systemic circulation and ally available on nursing units) or pharmacists when indicated. A filtered aspira- • IV flow rates are usually calculated in mL/hour and drops per tion needle should be used when withdrawing medication minute. Required information includes the amount of solution or from a vial or ampule, to remove any particles in the solu- medication to be infused, the time or duration of the infusion, and tion. The filter needle should then be discarded, to prevent the drop factor of the IV administration set to be used. The drop filtered particles from being injected when the medication is factor of macrodrip sets may be 10, 15, or 20 drops per milliliter, added to the IV fluid. The drop factor of all microdrip sets is • Check the expiration date on all IV medications. Following is a sample calculation: have a limited period of stability after they are reconstituted Order: Cefazolin 1 g IV q8h or diluted for IV administration. Most are compatible with 5% dextrose in water or Solution: Divide 100 by 60 to determine mL/min (1. CHAPTER 3 ADMINISTERING MEDICATIONS 39 In many settings, needleless systems are being used. These Nursing Notes: Apply Your Knowledge involve a plastic tip on the syringe that can be used to enter vials and injection sites on IV tubing. Needleless systems were developed Your client has a nasogastric feeding tube in place. You will be ad- ministering morning medications, including 4 tablets, 1 capsule, because of the risk of injury and spread of blood-borne and 10 cc of an elixir. Describe how you will safely administer pathogens, such as the viruses that cause acquired immuno- medications through a feeding tube to this client. When vials or ampules contain a powder able with or without an attached needle. Syringes are calibrated form of the drug, a sterile solution of water or 0. However, the chloride must be added and the drug dissolved before with- calibrations vary according to the size and type of syringe. Use a filter needle to withdraw the medication from Insulin and tuberculin syringes are used for specific an ampule or vial because broken glass or rubber fragments purposes.
She said she was allergic to or had be- come nauseated on every known pain medication symptoms 0f diabetes order 25 mg capoten visa. She knew them all by name and dosage and told me what each one did that was bad for her—skin rashes medicine 19th century order capoten pills in toronto, headaches symptoms torn meniscus 25mg capoten with visa, nausea, constipation, burning lips, itching legs, water- ing eyes, ringing ears, and many more symptoms that the pills that were supposed to help her had caused. After the first back operation, she could not walk for three months and then only with a cane. Tese complications were compounded by many of the drug reactions she had just listed. Between the first and second back operations, she had a mis- 144 Symptoms of Unknown Origin carriage and had to have a D and C (dilation and curettage) to stop the bleeding she had discovered in the middle of the night; she said she was nearly bleeding to death before they got me to the hospi- tal. She was so weak after the second back operation that her husband had to carry her in his arms around the house and to the bathroom. The third back operation had been a year before I saw her, and the numbness in both feet that followed that operation had just cleared up a few months ago. I would interrupt her to amplify details for each story and each com- plication or drug reaction. I left after the first visit, saying that I had a lot of things to think about and that I did not know what I would recommend. About this time in my search for new ways to deal with difficult patients like Regina, I had read a book called Change (Watzlawick, Weakland, and Fisch 1974) The authors described a patient very much like Regina who they posited liked to defeat experts. They mentioned a class of people who, for whatever reason, play a game of defeating experts. Tere is only one way that an expert (a clini- cian, in this case) can be defeated and help the patient at the same time, the authors suggest: a therapeutic paradox. According to the method described in Change, the patient (in this case, Regina) is saying unconsciously: No matter what you do, I will stay sick. You have heard all my old experiences with doc- tors, and in each one I did not get well. In fact, no matter what the A Paradoxical Approach 145 doctor did, I got worse. The therapeutic paradox the authors suggested is what I tried with Regina. I discussed the case with the orthopedist and he agreed with the approach I outlined. He had nothing to offer the patient and could think of no other tests or operations that would help. She had been in physical therapy for months with no help; in fact, she thought she had strained her back even further with some of the treatments. I asked the head nurse on the unit to be there and witness what I told Regina. I was very anxious because I had never been as frank as I intended to be with Regina, and I could not predict what reaction she might have. I intended to tell her exactly what I thought about her present condition and what I thought would happen to her in the future. I was going to follow the rules of the paradox, because I believed it was as close to the truth as I could get. If it did not, I could not imagine how it would hurt her except to make her angry. I recounted in great and slow detail all her previous operations and the complications and problems she had after each one. After I went over all the operations, I went on to the drugs and retold the side effects and toxic reactions she had told me about. I named all her previous doctors and what she said they had told her and how she thought each one was wrong and how each one had not helped but had indeed made her worse. I then went back over the physician list, naming each doctor 146 Symptoms of Unknown Origin who had seen her and what problems he or she had caused. And then I said something like this: I know some of these doctors, and they are fine physicians and surgeons. Why, I wonder to myself, do you think I would be any better than those you have seen. You are allergic to or you get sick with every known pain-re- lieving drug. Tere are no other tests, no other operations, no other drugs to recommend.
A patient who undergoes a total knee replacement should have less knee pain when he or she walks treatment hypercalcemia capoten 25 mg cheap, experience a good range of motion of the joint treatment zygomycetes purchase capoten overnight, and be able to perform the activities of daily living most of us take for granted 20 medications that cause memory loss 25 mg capoten free shipping, such as walking several miles, dancing, doing yard work, and performing normal household chores. Functional status is usually measured before and at several points following the treatment or procedure. For some surgical procedures, such as total joint replacement, it is common to obtain a baseline assessment prior to the procedure and then assessments at regular intervals following surgery, often at 1, 3, 6, and sometimes 12 months postoperative. The sur- vey can be collected by several means including mail or telephone and, most recently, on the Internet. The most widely recognized early pioneer of functional status sur- veys is John Ware, Ph. For many years, health plans have used a variety of means to collect data to report on their performance, track the manage- ment of the care received by their members, and direct programs in dis- ease management and care management. Because of this experience, health plan data have become more and more reliable. In fact, most health plans Data Collection 129 now have sophisticated data warehouses and a staff of expert data analysts. Because they contain detailed information on all of the care received by health plan members. When the bill is submitted to the health plan for payment, it is captured in a claim-processing system. As a result of this process, all of the care received by an entire population of patients, including hospitaliza- tions, outpatient procedures, physician office visits, lab testing, prescrip- tions, anything billed to and paid for by the health plan, is contained in the health plan claims database. From a population management perspec- tive, the health plan claims database is often the only source for all infor- mation on the care received by a patient and, for that matter, an entire population of patients. It is therefore an excellent source of data for dis- ease management programs where the goal is to improve the health for a specific population of patients. Not only does it provide a comprehensive record of patient activity but it can also be used to identify and select patients for enrollment into disease management programs. An excellent tracking tool for examining the entire continuum of care, claims databases are also the only externally available source of information for describing physician office practice. In essence, a claims database is the single best source of information on the total care received by a patient. Health plan databases are commonly used to identify patients who have not received needed preventive services such as mammograms, colon cancer screening, and immunizations. They can identify patients who are not receiving the appropriate medications for many chronic medical con- ditions such as heart failure or asthma. Many of the same considerations covered under hospital administrative databases apply to health plan databases, including questions associated with accuracy, gran- ularity, and timeliness. Provider-Specific Data Report ADA In Criteria Standards Points Tested Standard Percent Education 1 / 2 year 48 42 42 88 Eye exams Annual 48 30 30 63 GlycoHb ordered Annual 48 45 45 94 GlycoHb level ≤ 7. Percent of Patients Within Standard 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Educ Eye Glyco Glyco LDL LDL Micro Micro Exam Lvl Ord Lvl Ord > 30 Ord Rx Filled Provider Med Group FIGURE 6. High-Risk Patient Detail—Patients Outside ADA Standards in Current Quarter (continued) Criteria for inclusion—one or more of the following: (1) no education in last two years; (2) no eye exam in last one year; (3) GlycoHb > 7. Education Exam Ordered Level Ordered > 30, Rx Filled Ordered Result Patient 100-319-xxx 7/21/99 7/15/99 6. Loeb Performance measurement is undertaken to meet multiple internal and external needs and demands. Internal quality improvement literature iden- tifies three fundamental purposes for conducting performance measure- ment: (1) assessment of current performance, (2) demonstration and verification of performance improvement, and (3) control of performance. These purposes of measurement are designed to complement and support internal performance-improvement activities. The first step in a structured performance-improvement project is to assess current perform- ance. This assessment assists in the identification of the strengths and weak- nesses of the current process, thereby helping to identify areas for intervention. It also provides the baseline data against which future meas- urement data will be compared after interventions have been implemented. The comparison of postintervention measurement data to baseline data will demonstrate and verify whether the intervention was an improvement. Measurement for control of performance is intended to provide an early warning and correction system that will highlight any undesirable changes in process operations. This is critical to sustaining the improvements that have been realized through process-improvement activities.
I was so tired of gasping for air during my workouts with David that I had to cut back chi royal treatment order capoten pills in toronto. THE ULTIMATE BODY 14-DAY PLAN 175 TLFeBOOK 176 THE ULTIMATE NEW YORK BODY PLAN TLFeBOOK DAY 11 Remember the ultimate rules of nutrition treatment of gout generic 25 mg capoten with mastercard. Drinking sufficient amounts of water is an essential part of this program and will assist your body as it gets rid of toxins and other impurities treatment high blood pressure cheap capoten 25mg with visa. Often the best response to this type of soreness is muscle movement through exercise. Movement, proper hydration, and nutrition are the perfect remedies for soreness and should keep you motivated, mobile, and productive. If you real- ly want to pamper yourself and continue to move forward in the right direction, sign up for a massage—and keep your exercise appointment intact. THE ULTIMATE BODY 14-DAY PLAN 177 TLFeBOOK ULTIMATE SUCCESS Name: Bonnie Berkovits Residence: New York, New York Occupation: Customer care manager Age: 46 Weight Lost: 10 pounds Other Accomplishments: Shrunk 3 inches from her waist, 4 1/ inches from 2 her bust, 3 inches from her hips, 1 inch from her thighs, and 1/ inch from 2 her arms. Comments: With a classic apple-shaped body, Bonnie needed to lose about 40 pounds. Also, with little exercise experience under her belt, the program started a little tediously. She was steadfast in her determination to handle all that I presented to her. Unlike some of my other clients, she welcomed the diet and did not feel deprived at all. After years of yo-yo dieting, she is finally on the way to achieving her fitness goals. I told David I felt ready to finally lose the extra 40 pounds I had gained during the past 10 years and to change my diet for the better. Complacency leads to lethargy and lethargy to disappointment and failure. Stay sharp, stay focused, and keep your eye on the prize: your transformed body. That should be enough incentive and motivation to take you through the next 48 hours of the program. As your punishment (yes, drinking is definitely taboo), you must complete 15 to 30 additional minutes of cardiovascular exercise. Make sure to hydrate with lots of water (even more than you would ordinarily drink) and take plenty of vitamins, minerals, and, in particular, milk thistle to cleanse your liver. When all is said and done, you will be a sweaty mess, but you will definitely have worked toward ridding yourself of the alcohol in your body. ULTIMATE SUCCESS Name: Galaxia Barraza Residence: New York, New York Occupation: Mom, public relations and casting specialist Weight Lost: 9 pounds Other Accomplishments: Shrunk her waist by 4 1/ inches and her thighs 2 and hips by 1 inch. Comments: Gali had given birth to a baby girl just four months before start- ing the program and had not exercised before, during, or since the pregnancy. Building up her cardiovascular stamina and strength endurance were key components to her success. By the end of the program, Gali could exercise aerobically for 45 minutes to an hour and had switched from her usual diet of rice and potatoes to one of vegetables, chicken, fish, salads, and protein shakes. I never watched what I ate, nor THE ULTIMATE BODY 14-DAY PLAN 181 TLFeBOOK did I exercise. During my pregnancy, however, I craved sweets and gave into my temptations. Although this certainly was an adjustment for me, the food was really good, and my cravings for carbs went away after three to four days. If you agree and can relate to these sentiments, then challenge yourself further by adding an additional 30 to 45 minutes of car- diovascular exercise to your regimen. You are on your way to completing the 14-day program with flying colors, and it will definitely be easier than it was last week.
Buy generic capoten canada. 05. SHINee - Sherlock - The Reason [LYRICS/MP3/DL].