
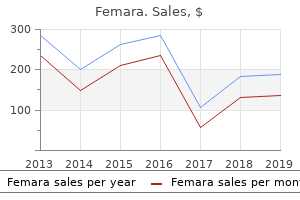
Femara
"Cheap femara 2.5 mg line, women's health clinic fort hood".
By: K. Jarock, M.S., Ph.D.
Clinical Director, Boston University School of Medicine
It can be seen how one basic infusion pump chassis can thus be made to give rise to effectively many different devices according to the micro- processor confguration menstrual joy buy femara without prescription. Each confguration or mode of use has its own attendant hazards in addition to those From container To patient general to infusion pumps women's health clinic saginaw mi generic femara 2.5 mg. Although all functionalities may be available in the one device breast cancer 2014 discount femara 2.5 mg mastercard, for risk management they may be selectively disabled through a restricted access menu such that only facilities that are needed in a clinical area are available to the user. Modern devices are also able to communicate with cen- tralized automated data archiving systems to automati- cally record the administration rate of a drug alongside the output of patient physiological monitors. Simple infusion systems In the operating theatre where there is closer observation Deliver of the patient’s hydration and circulating volume as neces- sitated by their rapidly changing status, most intravenous fuids are still administered under gravity from fexible Figure 19. These are of several types: • simple fuid administration, no flter, droplet size • simple infusion rate with an additional bolus approximately 15 drops/ml (0. These giving sets use • the in-built processor (or an additional piggybacked a larger-bore tubing and a double drip chamber processor) can contain algorithms for the containing a foat: by squeezing the bottom pharmacokinetics of particular drugs, allowing chamber, the foat jams the inlet and acts as a automated drug delivery based on achieving any one-way ball valve allowing fuid to be pumped. These systems are currently only commercially A fap or ball valve at the bottom of the burette available for use in anaesthesia and are principally prevents air entering the drip chamber when the limited to four drugs: propofol, remifentanil, burette is empty sufentanil and alfentanil. Patient variables such as • platelet giving sets, designed to reduce the risk of age, sex, weight and height may need to be inputted aggregation in the giving set as would occur with to complete the algorithm. This neces- should be made for warming them to body temperature, sitates a narrower-bore tube made from softer plastic to otherwise signifcant cooling of the body may ensue (see function with the peristaltic pumps (see below). These sets usually have a 15 µm flter at the base of the drip chamber and are not suitable for infusing blood or for use in adult resuscitation. Hence, they have to be powered by • occlusion of the tubing from a rate controlling some form of motor, which must be coupled to a mecha- device nism for driving the fuid • the physical properties (i. The driving force in the majority of infusion pumps and The manufacturers of giving sets quote the size of drops electronic syringe drivers is provided by an electronic as number of drops per millilitre, usually between 10 and stepper motor, which is directly controlled from a digital 60, but it must be remembered that the actual volume of microprocessor system. It is, therefore, diffcult, without electronic feedback, to control such a motor accurately. This, like the newer peristaltic pumps, is driven by a stepper motor con- Anvil plate ‘Pinched off’ volumes trolled directly by a microprocessor. The volume of the cassette is typically about 5 ml, with the dedicated dispos- Figure 19. A valve operating in harmony with the piston directs fow from the infusate bag to the reservoir or from there to the patient. Precision silicone tubing is drawn rapidly from the reservoir bag into the cassette in often used in this section of the giving set. The valve is then actuated such that on the Rotary peristaltic pumps are now more often seen in use piston upstroke the contents are expelled at the required for the less demanding requirements of enteral feeding rate into the patient, and the cycle is repeated. The driving force is again a These are seen much less frequently now owing to the stepper motor. The rotary motion from the motor is trans- expense of the disposables and the feasibility of getting lated into a linear peristalsis by the use of cams and cam good accuracy using simple intravenous giving sets in followers as shown in Fig. Because such infusion pumps have the theoretical capacity to inject limitless quantities of air into a patient Peristaltic pumps should air ingress occur upstream of the pump (for The principle of the peristaltic infusion pump is shown in example due to an empty infusion bottle), these devices Fig. The tubing of a giving set is compressed by a incorporate sophisticated ultrasonics (Fig. These are usually mechanism must be hard wearing, of known and consist- placed downstream of the pump mechanism. Further pro- ent internal volume, and have no memory after compres- tection is conferred by setting target delivery volumes sion so that it easily flls on being released. Thus, each pulse applied to the stepper 0 10 20 30 40 50 60mm motor causes the advancement of the syringe plunger by Set rate 10 bleeps mm per (24 h) day a known amount. Syringe pumps (the term is synonymous with syringe of the pressure generated in the infusion line beyond the drivers) are now designed to automatically recognize a device. Peristaltic intravenous pumps, therefore, use a variety of syringes by virtue of the calibre of the barrel sensing piston pressing on the infusion line immediately using some form of spring-loaded arm; some manufactur- downstream of the pumping chamber. This is calibrated ers’ models nonetheless require manual confrmation of to indirectly measure line pressure and can be programmed the detector. Infusion line pressure (and empty syringe to alarm for occlusion at different pre-set levels. This Syringe drivers is a more popular option than the use of specialized infu- There continues to be a range of small simple battery- sion sets with in-built diaphragm and corresponding operated syringe drivers (Fig.
A large nontender gallbladder is often indicative of gallbladder hydrops (due to a cystic duct stone) or an obstructed common duct by a neoplasm (Courvoisier gallbladder) women's health center at evergreen buy femara 2.5 mg online. In the latter instance menopause quizlet purchase femara amex, there is always jaundice women's health issues in malaysia order 2.5mg femara fast delivery, whereas in the former instance, there is not. Now, it is necessary to look for systemic signs of cirrhosis (spider angiomata, palmar erythema, gynecomastia, testicular atrophy, ascites, caput medusae, and hemorrhoids). One should be sure to look for the Kayser–Fleisher ring in the cornea in Wilson disease and the bronze skin in hemochromatosis, not to mention xanthelasma and tendon xanthoma in biliary cirrhosis induced by 49 hyperlipemia. Neck Mass Differentiating a neck mass that is thyroid tissue from an enlarged lymph node or other mass is no problem. A diffuse thyroid mass can be further identified as Graves disease by looking for tremor, tachycardia, and exophthalmos. A toxic adenoma can be differentiated from a nontoxic nodule in a like manner, except the exophthalmos is not as pronounced. Another neck mass that moves when the patient swallows is the thyroglossal duct cyst, but it is always in the midline. It is possible to distinguish a Zenker diverticulum by noting the increase in size when the patient swallows liquid. The experienced clinician knows that a metastatic neoplasm of the cervical lymph nodes can be differentiated from Hodgkin disease by the fact that the metastatic neoplasm is hard whereas the lymph node hypertrophy of Hodgkin lymphoma is softer and rubbery. Transillumination may be used to help differentiate a colloid cyst of the thyroid and a thyroglossal cyst, but a negative result does not rule out either condition. Scrotal Mass Transillumination is extremely useful in distinguishing a hydrocele from a hernia or testicular tumor. A varicocele can be distinguished by the fact that it disappears when the scrotum is raised above the abdomen. A hernia can be diagnosed by the fact that it is reducible unless it is incarcerated. One other sign of a hernia is that the physician cannot “get above” the swelling (i. Torsion of the testicle can be differentiated from orchitis by the relief of pain on elevating the testicle in torsion. Splenomegaly Massive splenomegaly is typical of three conditions: kala azar, chronic myelogenous leukemia, and myeloid metaplasia. The best way to examine for an enlarged spleen is to have the patient lie on his or her right side with knees flexed almost onto the abdomen, place the fingers of one’s left hand under the subcostal margin, and have the patient take deep breaths. It may be necessary to have the patient take several breaths before the physician is 50 sure that he or she is feeling the splenic margin. Another way to verify clinically that a patient has an enlarged spleen is to do a tourniquet test because there is often a thrombocytopenia. Also, look for hepatomegaly because hepatosplenomegaly is common in many diseases (e. Most of these are related to bleeding from Little area in the anterior nasal septum, and packing or cautery is a simple solution. However, when a patient experiences recurrent attacks of epistaxis, the examination must be more thorough and extensive. The physician should check the blood pressure and eye grounds for evidence of hypertension. Careful examination of the nasal passages for allergic rhinitis, a granuloma, or neoplasm is important. Hematemesis and Melena Surely a physician is going to consult a gastroenterologist and prepare the patient with hematemesis and/or melena for endoscopy; however, one can help the gastroenterologist by looking for signs of cirrhosis such as caput medusae, hemorrhoids, ascites, jaundice, hepatosplenomegaly, spider angiomata, palmar erythema, and so on. In addition, look for signs of hereditary telangiectasia on the tongue and mucous membranes. Hematuria Careful examination of the flanks for a mass (neoplasm, hydronephrosis, polycystic kidney disease) or tenderness (pyelonephritis or renal calculus) is important. It should go without saying that a thorough pelvic and rectal examination must be done. The physician should look for signs of bleeding elsewhere, and in addition to ordering a coagulation profile, he or she should not forget to do a Rumpel–Leede test. If these techniques fail to yield the answer, the physician examines the nasal passages for the source.
Enteral nutrition as a primary therapy for intestinal lymphangiectasia: Value of elemental diet and polymeric diet compared with total parenteral nutrition breast cancer 2014 products cheap 2.5mg femara amex. Primary intestinal and thoracic lymphangiectasia: A response to antiplasmin therapy breast cancer 60 mile walk atlanta cheap femara 2.5mg overnight delivery. Type I intestinal lymphangiectasia treated successfully with slow-release octreotide menopause stages purchase generic femara. Corticosteroid-responsive intestinal lymphangiectasia secondary to an infammatory process. Analysis of fat and muscle mass in patients with infammatory bowel disease during remission and active phase. Growth failure and infammatory bowel disease: Approach to treatment of a complicated adolescent problem. Growth, body composi- tion, and nutritional status in children and adolescents with Crohn’s disease. Nutritional considerations and management of the child with infammatory bowel disease. Nutrition support for pediatric patients with infammatory bowel disease: A clinical report of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Journal of Bone and Mineral Research: The Offcial Journal of the American Society for Bone and Mineral Research. Nutrition in Clinical Practice: Offcial Publication of the American Society for Parenteral and Enteral Nutrition. Dairy sensitivity, lactose malabsorption, and elimination diets in infammatory bowel disease. Report on the vitamin D status of adult and pedi- atric patients with infammatory bowel disease and its signifcance for bone health and disease. Improved outcomes with quality improve- ment interventions in pediatric infammatory bowel disease. Vitamins A and E serum levels in children and young adults with infammatory bowel disease: Effect of disease activity. Low serum and bone vitamin K status in patients with longstanding Crohn’s disease: Another pathogenetic factor of osteoporosis in Crohn’s disease? Serum transferrin receptor in children and adolescents with infammatory bowel disease. Oral ferrous fumarate or intravenous iron sucrose for patients with infammatory bowel disease. Intravenous iron sucrose versus oral iron sup- plementation for the treatment of iron defciency anemia in patients with infammatory bowel disease—A randomized, controlled, open-label, multicenter study. Chronic intermittent elemental diet improves growth failure in children with Crohn’s disease. Improved growth and disease activity after intermit- tent administration of a defned formula diet in children with Crohn’s disease. Enteral nutrition and cortico- steroids in the treatment of acute Crohn’s disease in children. Exclusive enteral feeding as primary therapy for Crohn’s disease in Australian children and adolescents: A feasible and effective approach. Nutritional supplementation with polymeric diet enriched with transforming growth factor-beta 2 for children with Crohn’s disease. How effective is enteral nutrition in inducing clinical remission in active Crohn’s disease? Meta-analysis of enteral nutrition as a primary treatment of active Crohn’s disease. Polymeric enteral diets as primary treatment of active Crohn’s disease: A prospective steroid controlled trial. A British Society of Paediatric Gastro- enterology, Hepatology and Nutrition survey of the effectiveness and safety of adali- mumab in children with infammatory bowel disease. Increasing incidence of Clostridium diffcile–associated diarrhea in infammatory bowel disease.
Body Composition Norms There are no universally accepted norms for body composition; however women's health vancouver bc buy generic femara online, Tables 4 menstruation quality buy cheapest femara and femara. A consensus opinion for an exact percent body fat value associated with optimal health risk has yet to be defined; however menstruation 1 cheap 2.5mg femara mastercard, a range of 10%–22% and 20%–32% for men and women, respectively, has long been viewed as satisfactory for health (71). More recent data support this range, although age and race, in addition to sex, impact what may be construed as a healthy percent body fat (35,58). Performance of exercise at this level of physical exertion depends on the integrated physiologic and functional state of the respiratory, cardiovascular, and musculoskeletal systems. This variable is typically expressed clinically in −1 −1 −1 relative (mL · kg · min ) as opposed to absolute (mL · min ) terms, allowing for meaningful comparisons between/among individuals with differing body −1 weight. O2max is the product of the maximal cardiac output ( ; L blood · min ) −1 and arterial-venous oxygen difference (mL O · L blood2 ). Significant variation in O2max across populations and fitness levels results primarily from differences in ; therefore, O2max is closely related to the functional capacity of the heart. The designation of O2max implies an individual’s true physiologic limit has been reached, and a plateau in O may be observed between the final2 two work rates of a progressive exercise test. Peak O (2 O2peak) is used when leveling off of O does not occur, or maximum performance appears limited by local2 muscular factors rather than central circulatory dynamics (75). Open circuit spirometry is used to measure O2max during a graded incremental or ramp exercise test to exhaustion, also called indirect calorimetry. In2 2 addition, the use of open circuit spirometry during maximal exercise testing may allow for the accurate assessment of an anaerobic/ventilatory threshold and direct measurement of O2max/ O2peak. Many automated systems are currently available that provide ease of use and downloadable data of test results that save time and effort; however, system calibration is essential to obtain accurate results (82). Administration of the test and interpretation of results should be reserved for trained professional personnel with a thorough understanding of exercise science. Because of costs associated with the equipment, space, and personnel needed to carry out these tests, direct measurement of O2max may not always be possible. When direct measurement of O2max is not feasible, a variety of maximal and submaximal exercise tests can be used to estimate O2max. These tests have been validated by examining (a) the correlation between directly measured O2max and the O2max estimated from physiologic responses to submaximal exercise (e. It should be noted that there is the potential for a significant underestimation or overestimation of O2max by these types of indirect measurement techniques. Overestimation is more likely to occur when (a) the exercise protocol (see Chapter 5) chosen for testing is too aggressive for a given individual (i. Every effort should be taken to choose the appropriate exercise protocol given an individual’s characteristics and handrail use should be minimized during testing on a treadmill (82). Maximal versus Submaximal Exercise Testing The decision to use a maximal or submaximal exercise test depends largely on the reasons for the test, risk level of the client, and availability of appropriate equipment and personnel (see Chapter 5). Maximal tests require participants to exercise to the point of volitional fatigue, which may be inappropriate for some individuals and may require the need for emergency equipment (see Appendix B). This information can be used to evaluate submaximal exercise responses over time in a controlled environment and make modifications the Ex R. Cardiorespiratory Test Sequence and Measures After the initial screening process, selected baseline measurements should be obtained prior to the start of the exercise test. The exercise test should begin with a 2–3 min warm-up to acquaint the client with the cycle ergometer or treadmill and prepare him or her for the exercise intensity in the first stage of the test. A specific protocol should consist of 2- or 3-min stages with appropriate increments in work rate. An appropriate cool-down/recovery period should be initiated consisting of either a. Continued exercise at a work rate equivalent to that of the first stage of the exercise test protocol or lower or b. A passive cool-down if the subject experiences signs of discomfort or an emergency situation occurs 11.
Cheap 2.5mg femara with mastercard. Diet Talk - Top Five Diet Tips for Pregnant Women.